
Update October 9th – ABC Media Watch, Northern Star HPV headline wrong
Just under a week ago The Northern Star published a one sided article alleging that a healthy 16 year old female was stricken with a host of physical ailments following administration of “the Gardasil vaccine”.
This specific claim is unverified in that conclusive evidence or clinical diagnoses pointing to Gardasil are absent. More so, from the viewpoint of international epidemiology, the two complex syndromes identified are not accepted as vaccine injuries caused by Gardasil. Toward the end of the article, Teen left in wheelchair after Gardasil HPV ‘reaction’, readers are informed that Olivia Odey (now 18);
…believes her symptoms were linked to a reaction to the Gardasil vaccine against cervical cancer, which the teenager had a few weeks prior to the onset of her symptoms.
No doubt given the weight of peer reviewed literature on the topic, and evidence offered in the article, Ms. Odey is indeed left with only her “belief”. Initially after presenting to hospital, “all tests came back normal”.
“I definitely think there was a link, but there’s no way to prove it,” Ms Odey said, admitting the proposition was controversial and “brushed aside by medical professionals”.
According to the Australian HPV vaccine website, for every million doses of the vaccine given there are only around three serious allergic reactions.
Adverse Events Following Immunisation are not “brushed aside” by Australian medical professionals. Regrettably, the article does not cast the profession in a favourable light and Ms. Odey reports, “a frustrating battle with the conventional medical system”.
“They wanted to send my mum and I across the road to a mental institution and told me ‘if there was a fire you would run right out of here’.
Ms. Odey apparently experienced photo-phobia, numbness, shingles, food allergies, tingling, joint pain, lethargy and discolouration of the legs. But it was heart palpitations that led her mother to contact a cardiologist in Auckland. The cardiologist referred her to a “specialised pain doctor”. She was diagnosed within an hour and began treatment the next day. Olivia Odey had been diagnosed with Complex Regional Pain Syndrome (Fact Sheet), also known as Reflex Sympathetic Dystrophy and Central Neural Sensitisation Syndrome [Central Sensitisation] (Physiopedia videos).
We should note with respect to diagnosing CRPS;
There is no diagnostic test for CRPS. Diagnosis is based on a person’s medical history and their symptoms. Sometimes, a doctor may order blood tests, bone scans, x-rays, CT scans or MRI scans to rule out other conditions that have similar symptoms.
Thus being diagnosed within an hour and beginning treatment within a day is seemingly unusual to say the least. Ms. Odey’s entire recovery is unusual. We’re informed neuroplasticity explains;
To come off the pain drugs Ms Odey did a three-day course on how to “retrain your brain pathways and change your physiology just by changing your thoughts and beliefs.”
CRPS is classified as a Rare Disorder and whilst there is a significant range of symptoms and intensity, factors relating to causation include trauma such as a fracture, forceful injury, crush injury, amputation, stroke, and spinal cord injury. Other disorders may predispose to CRPS;
However, it has become increasingly clear that it plays a role in many different chronic pain disorders. It can occur with chronic low back pain, chronic neck pain, whiplash injuries, chronic tension headaches, migraine headaches, rheumatoid arthritis, osteoarthritis of the knee, endometriosis, injuries sustained in a motor vehicle accident, and after surgeries. Fibromyalgia, irritable bowel syndrome, and chronic fatigue syndrome, all seem to have the common denominator of central sensitization as well. […]
What isn’t clear in Ms. Odey’s case is if these possible causes were ruled out before blaming Gardasil.
Of great significance is that;
A prior history of anxiety, physical and psychological trauma, and depression are significantly predictive of onset of chronic pain later in life. […] The onset of pain is often associated with subsequent development of conditions such as depression, fear-avoidance, anxiety and other stressors.
Again it isn’t clear if all possible contributing stressors were ruled out.
The table below summarises the range of symptoms associated with CRPS.
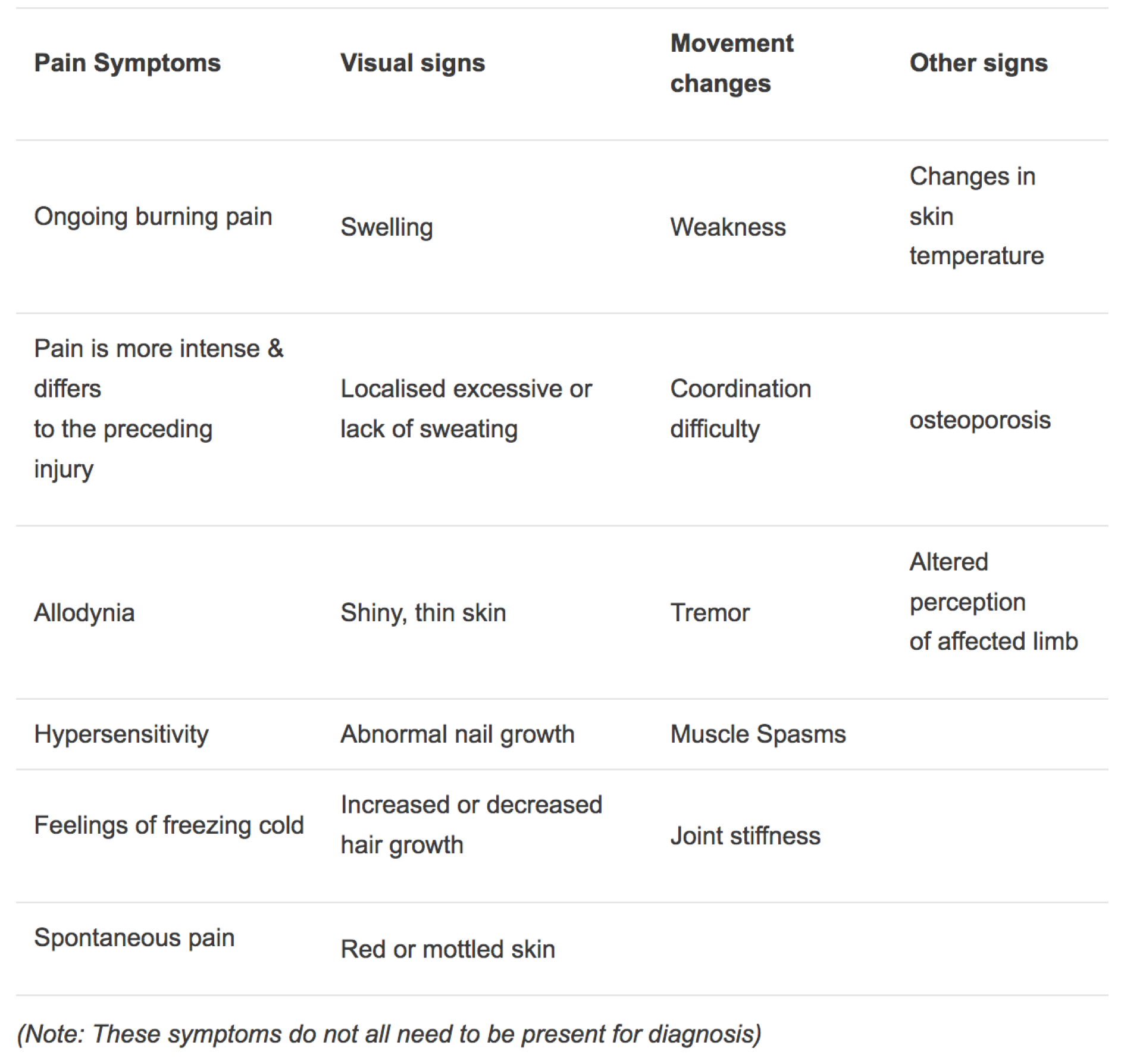
Source: Australian Pain Management Association
Given the complications listed in the above table one can appreciate the slow progression of physical therapy outlined below.
Desensitization – “to hurt is not to harm”. Over a period of time the person with CRPS will be encouraged to desensitize the affected limb so that the hypersensitivity and allodynia is reduced. For example, over a period of three years Annette, a CPRS patient, began with moving a silk scarf over her foot, progressed to being able to wear a foot stocking, to a sock, sandal and finally a closed in shoe for a short period. This process took three years but improvements are still being made.
Graded motor imagery (GMI) combined with medical management is recognized as being effective in reducing pain in CRPS. GMI involves encouraging the person to differentiate between left and right limbs to re-establish right and left concepts in the brain. Progressively, a mirror box is introduced. The person is asked to watch the mirrored image of the unaffected limb moving in the mirror. Then, the person moves the affected limb in the mirror box while watching the mirrored image of the unaffected limb. This tricks the brain into thinking it is seeing the limb with CRPS moving without pain.
Finally we can find comprehensive refutation of the notion that HPV vaccination causes Regional Pain Syndrome and Central Sensitisation from reputable sources in the literature. A Safety Study of Gardasil 9 in PRISM/Sentinel using sequential analysis, is worth consulting. Version 2 was published only three days ago – September 27th 2017. Page 2 contains the paragraph on Complex Regional Pain Syndrome. Following a clinical description of CRPS the paragraph continues (italics and bold mine);
In June 2013, the Japanese Ministry of Health, Labor, and Welfare suspended its recommendation of routine immunization with HPV vaccine in girls and women following post-vaccination reports of serious chronic pain and concern about a possible association with HPV. In early November 2015, the European Medicines Agency’s Pharmacovigilance Risk Assessment Committee completed a detailed scientific review of the evidence related to a possible association between HPV vaccines and CRPS. The Committee concluded that the evidence did not support a causal link between the vaccines and the syndrome. Although U.S. vaccine safety information sources such as the Vaccine Adverse Event Reporting System (VAERS) have not suggested an increased risk of CRPS following HPV vaccination either, some post-HPV-vaccine cases have been reported to VAERS.
Much has been made of the Japanese suspension of HPV vaccination due to post-vaccination reports of serious chronic pain and concern about a possible association with HPV. Interestingly if we follow the link above to version 2, we find that the citation to these post vaccination reports is; Kinoshita T, Abe RT, Hineno A, Tsunekawa K, Nakane S, Ikeda S. Peripheral sympathetic nerve dysfunction in adolescent Japanese girls following immunization with the human papillomavirus vaccine. Intern Med. 2014;53:2185-200.
To better understand the reliability of the report of Kinoshita et al, we should consult the 2017 critique, Tackling Antivaxers in the Literature by David Hawkes, Joanne Benhamu and Julia Brotherton. Whilst a number of examples are addressed in this publication it is the widespread criticism of Kinoshita et al and the subject of peripheral sympathetic nerve dysfunction following the HPV vaccine that is significant.
The Introduction reads;
To understand strategies used by Human Papillomavirus (HPV) vaccine critical authors, exemplified by a recent publication in the Nature published journal, Scientific Reports, to produce a false evidence base in the peer reviewed scientific literature.
Methods;
Critical analysis of anti (HPVE) vaccine papers, including retracted articles, links between authors of these papers and conflicts of interests, journals used to publish these papers, self citations and dissemination of these articles and associated commentary on social media.
HPV Vaccination: Japan;
Several publications have been produced by Japanese authors critical of HPV vaccination. In 2014, Kinoshita et al published a paper entitled “Peripheral Sympathetic Nerve Dysfunction in Adolescent Girls following Immunization with the Human Papillomavirus Vaccine” in Internal Medicine (a small journal with an impact factor of less than 1). To date it has been cited over 40 times. Despite several (published) letters of concern highlighting errors in the paper from highly respected researchers in the field the manuscript remains available. A recent publication by Aratani et al in the Nature published journal Scientific Reports has caused similar concern and is currently under review by the journal. This case garnered a much wider audience and an article highlighting concerns was featured in Science. This suggests that scientists are being more proactive in combatting bad HPV vaccination science.
In July last year Outcomes for girls without HPV vaccination in Japan was published in the Lancet. The author’s final paragraph read;
Sadly, Japan’s failure to provide HPV vaccination for young women has now become a global concern. Similar trends are occurring in countries outside of Japan, which will lead to increased incidences of HPV-related cancers. Although further efforts are required to overcome the many barriers leading to decreasing cervical cancer mortality, many challenges remain.
A comprehensive summary of the paper is available here, Lack of vaccinations increased risk of HPV infections in Japan;
Japanese women who became adolescents between 1993 and 2008, a period in which vaccination against cervical cancer was temporarily suspended, are at higher risk of having HPV16/18 infection, which is known to trigger the onset of cervical cancer. However, the infection risk can be decreased if vaccination is re-established. […]
The authors strongly recommend that HPV vaccination encouragement is resumed before the end of 2016, to reduce the risk of future infection in different age groups and to ensure all women will receive protection against cervical cancer.
As time progresses there continues to be a lack of evidence that may be considered as verification that HPV vaccines are causally linked to the conditions mentioned by Olivia Odey and described by Alina Rylko in The Northern Star article. Ms. Odey is heading to Byron Bay to begin a health blog. Yet in the present climate in which Australian vaccine safety and efficacy has been attacked by organised anti-vaccine lobbyists the tone of the article seems patently irresponsible.
The present consensus holds that CRPS and Central Sensitisation occur at levels expected of the populations effected. Evidence doesn’t support a causal link between the vaccines and the syndrome. Reports following HPV vaccination are consistent with what is expected for the age group. No fact sheets specific to these conditions list any vaccination as a cause or a predisposing condition. Data will continue to be gathered.
As yet there is no conclusive evidence to support Ms. Odey’s “belief” that Gardasil caused her condition.
———————————————————————
- Another condition for which HPV vaccination has been blamed is Postural Orthostatic Tachycardia Syndrome (POTS).
- HPV vaccination and complex regional pain syndrome: lack of evidence
- HPV Vaccines: EMA confirms evidence does not support that they cause CRPS or POTS
- Investigating reports of CRPS: An analysis of HPV 16/18-Adjuvanted vaccine post-licensure data (GSK investigation)
- The first few minutes of the video below from the EMA begins to outline the lack of evidence between HPV vaccination, CRPS and POTS.
- Central sensitisation in chronic pain
- Complex Regional Pain Syndrome
European Medicines Agency (EMA) virtual press briefing – Human papillomavirus (HPV) vaccines
