
- What is VAERS?
- OpenVAERS
- VAERS Underreporting
- What antivaxxers won’t tell you
- Antivax Winning Formula
- Conclusion
Since the inception of VAERS, anti-vaccination activists have misused reports as a cornerstone in their campaign to misinform and mislead. Vaccination against COVID-19 has led to that misuse exploding.
What is VAERS?
VAERS is the U.S. based Vaccine Adverse Event Reporting System managed by the Department of Health and Human Services (HHS) and co-managed by the Centers for Disease Control (CDC). It is an early warning system that collates reports of suspected adverse events following immunisation. A full explanation is here. Reports may be submitted by anyone who has received a vaccine authorised in the United States. Doctors, health workers, family members and associates can also submit reports. It is an open passive reporting system that allows reports from anyone who is aware of an adverse event they perceive as related to a vaccine.
It follows that the reports are just that; reports. Reports that contain no information about causality or indeed accuracy. This is not to say they are inaccurate. Rather that their true meaning, and indeed impact, can only be borne out in the context of further evaluation. Evaluation will assess any pattern of events, related health problems, any identifiable mechanism of causality and the time frame between vaccination and adverse event. Suspect vaccines would be suspended and emergency investigations employed to assess the scale and seriousness of adverse reaction(s). If the adverse event is confirmed to be more significant than in pre-licencing trials, the vaccine is removed from market.
Research and peer reviewed publication would follow, describing these findings. This information is of enormous benefit to the design, manufacture and trial of future vaccines. What stands out immediately is that determining adverse events due to vaccination requires significant input seperate from VAERS. The most important and irrefutable element about VAERS reports is that they do not represent cause and effect.
The VAERS site includes a Guide to Interpreting VAERS Data.
Under Evaluating VAERS Data:
When evaluating data from VAERS, it is important to note that for any reported event, no cause-and-effect relationship has been established. […]
VAERS collects data on any adverse event following vaccination, be it coincidental or truly caused by a vaccine. The report of an adverse event to VAERS is not documentation that a vaccine caused the event.
Under VAERS Data Limitations:
Reports vary in quality and completeness. They often lack details and sometimes can have information that contains errors. […]
No proof that the event was caused by the vaccine is required in order for VAERS to accept the report. VAERS accepts all reports without judging whether the event was caused by the vaccine.
The above is a small selection from the guide. Yet it is enough to inform readers seeking definitive information on adverse events linked to vaccines, that it will not be found there. Exploiting the reports to provide an accurate picture of potential or existing problems takes resources. Resources that individuals don’t have. Consider the case of RotaShield. This rotavirus vaccine was taken off the U.S. market in 1999 because of an association between the vaccine and intussusception. The U.S. Advisory Committee on Immunisation Practices (ACIP) voted for its removal after an in depth review of available data. RotaShield was available for just months.
Paul Offit is well schooled in how VAERS is misused. He is also a firm supporter of civilian reporting because, as intended, unanticipated side effects can be caught this way. He has referred to VAERS as a “hypothesis-generating mechanism”, and observed about RotaShield:
There were a number of VAERS reports that patients within a week developed an intestinal blockage. A study was done and it was shown to be a causal association. VAERS was the tipoff. There’s value in it.
Medscape provide detail on the scale of the study:
The suspected association between RRV-TV and intussusception based on a review of VAERS data led CDC, in conjunction with state and local health departments, to implement a case-control study [in 19 U.S. states among 429 infants and 1,763 matched controls] and case-series analysis and a retrospective cohort study [among 463,277 children].
So yes. If it’s confirmation of adverse events due to vaccination one seeks, merely perusing VAERS isn’t enough. This doesn’t stop antivaxxers from abusing the VAERS database to create the illusion of wide scale “vaccine injury”. As we’ve seen time and again during the COVID-19 vaccine rollout, screenshots and memes reach a large audience. Discredited Australian Instagram influencer and anti-vaccine advocate, Taylor Winterstein, has misused VAERS data to attack “mainstream mentality”. These tactics have the added advantage of side-stepping the guide to interpreting what is limited data on VAERS. The same approach is used by right wing cable news outlets. There are numerous techniques used to avoid the reality that there is only a temporal, and not a causal, relationship between vaccine and adverse reaction. Presenting government data carries a certain authority. Stripping it of context ensures it is inaccurate.
OpenVAERS
Post hoc ergo propter hoc: After this therefore because of this. This fallacy is the fuel driving the VAERS misinformation empire. Without it, outright claims cannot stand. Nor could the inference and extrapolation that comes from accepting widespread vaccine injury and death. The Vaxxed II bus in Australia is a typical example. It began last year, collecting dubious testimonials on “the vaccine-killed and injured”. Last month it began targeting the COVID-19 vaccine. Removing context from VAERS data ensures post hoc fallacy. This is exactly what the OpenVAERS project does. Launched in September 2019, it was initially run from archivist.net as confirmed on the Facebook page of The Archivist. In January 2021 the domain switched to openvaers.com and focused on COVID-19 vaccination data. Unsurprisingly OpenVAERS is a favourite of antivaxxers. Until recently, the index page offered:
The OpenVAERS Project allows browsing and searching of the reports without the need to compose an advanced search (more advanced searches can be done at medalerts.org or vaers.hhs.gov).
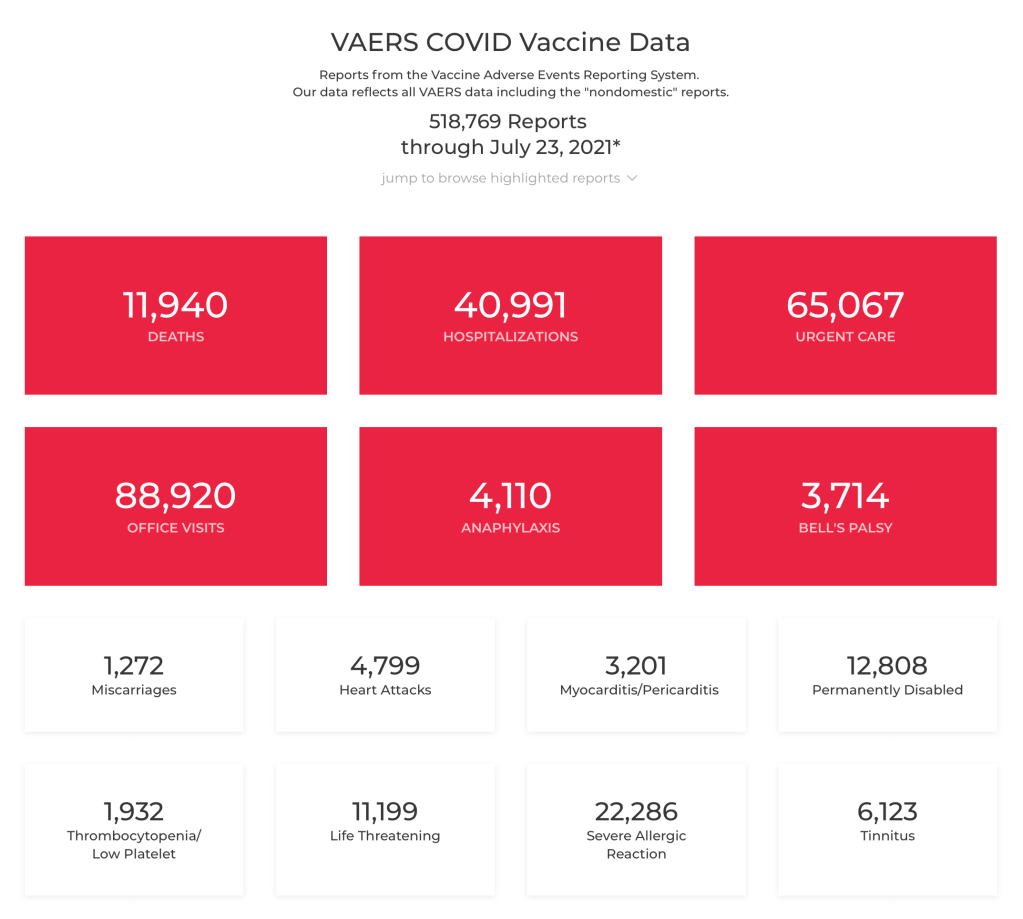
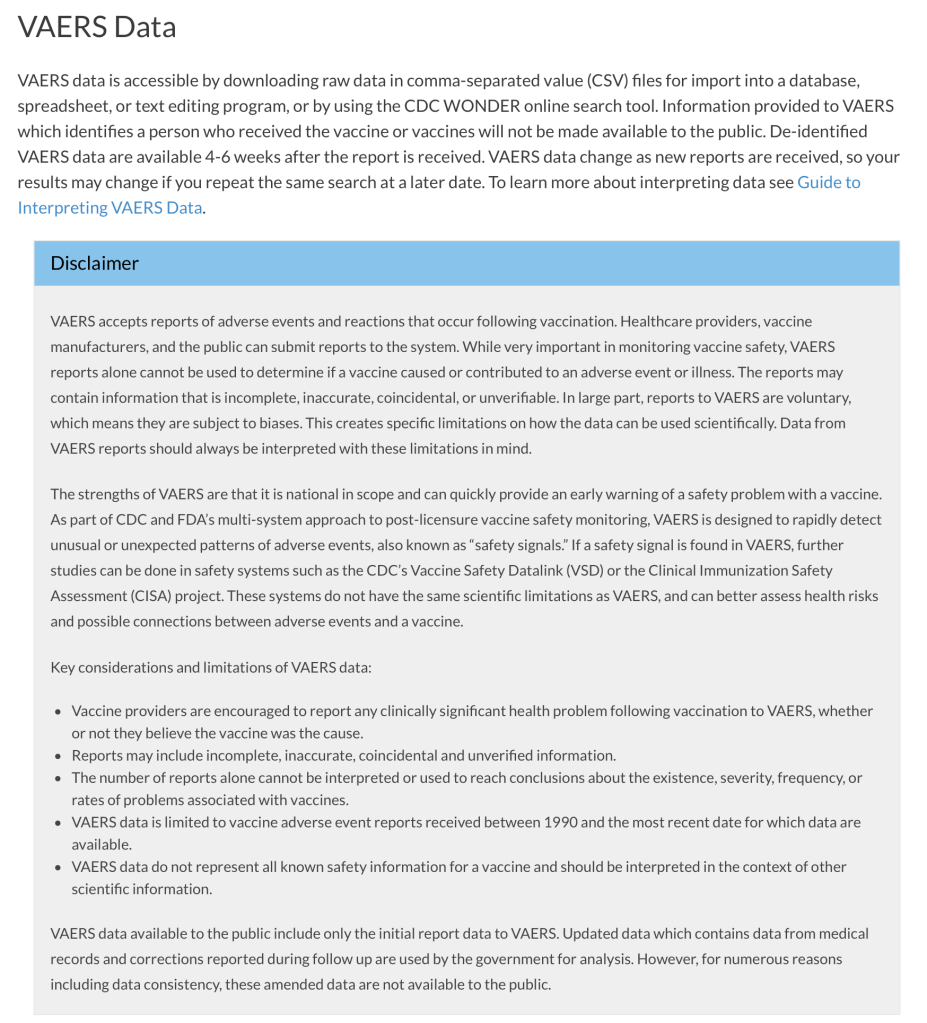
That’s what we find on the archived index page as at 1 August 2021. The next capture is 23 August 2021. At some time between these captures, OpenVAERS included a link to its own copy of the VAERS disclaimer both on the index page and its impactful VAERS COVID Vaccine Data page. The change on the vaccine data page was minor. Compare the 23 July and 20 August pages below. Keep in mind this is what readers see when they land on the data page. To appreciate the importance of context I’ve included a screenshot of the government VAERS data page.

Prior to this, users of OpenVAERS would have to navigate to the About page and follow the link to the VAERS About page. The change came just prior to the publication by Logically, a misinformation tracking group, of an article on 12 August which revealed the name and face behind the site. Logically had posed questions and a request for comment, which may have prompted the design change. Lizabeth Pearl Willner (below) better known as Liz Willner believes her daughter was injured by vaccination and began posting anti-vaccine content on social media in April 2019. She insists the site exists to provide easy access to official data.
There were significantly more visits to OpenVAERS (1.23 million) than to VAERS (796.63k) between February and July this year. Logically discovered that 30 percent of referrals to OpenVAERS are from the right wing, fake news site, Gateway Pundit. 10 percent are from conspiracy theorist Vernon Coleman (old man in a chair). These sites promote COVID conspiracies, pseudoscience and anti-vaccination rhetoric. Willner’s now deleted Facebook account and recently deactivated Twitter handle @1pissedoffmom1, amplified the reach and impact of OpenVAERS.

Until April 2021 OpenVAERS included a dedicated and searchable vaccine excipients table. The OpenVAERS blog now returns a 404 page. Indeed those behind OpenVAERS seem intent on having their deleted content also removed from archive.org. When running, the blog provided a one stop antivax shop for COVID-19 misinformation for “warrior moms, dads and grandparents”.
Call For Action posts contained alarming inaccuracies about the COVID-19 pandemic and the safety of the COVID-19 vaccine. The posts linked to ready-made PDFs to be printed out and mailed to “friends, family, and elected officials”. The drill, as they called it, was “10 copies, 10 stamps, 10 envelopes, 10 chances to wake someone up”.
As recently as 2 August this year we find:
Unfortunately, coronavirus vaccines excel at producing iatrogenic injury. Since their rushed introduction in December, these shots have produced four times more fatalities than the terrorist attacks on 9/11.
A link to that particular post, along with the 9/11 reference was shared on The Defender. That’s the “news and views” site of Robert F. Kennedy Jr.’s Children’s Health Defense. The potential for harm by encouraging vaccine hesitancy in the midst of a pandemic is significant. Willner has ignored requests for comment from VICE News. The OpenVAERS blog also claims to be getting around “the criminal censorship of essential vaccine information on social media”.
Successful misuse of data this way relies upon the base rate fallacy. When vast sections of the population are involved, background mortality and morbidity become significant. Adverse events and deaths are reported in such numbers not because the vaccine is responsible, but because so many people are being vaccinated on any given day. Each person is given literature on how to report adverse reactions to VAERS. The V-Safe initiative includes regular text messages asking about any symptoms or changes to health. Attention given COVID-19 vaccination is unparalleled and this is reflected in data. Reports to VAERS (CSV VAERS Data accessed 3 September 2021) for all of 2020 totalled 63,544. To date, reports for 2021 ending 20 August, total 674,382. Not only are these reports unconfirmed but the safety of the COVID-19 vaccine is regularly affirmed.
Kolina Koltai is a Postdoctoral Fellow at the Center for an Informed Public based at the University of Washington. She describes OpenVAERS as “misinformation 101” and stresses that such decontextualisation is common to misinformation. Koltai uses such examples in classes that she teaches. In responses to questions posed by Logically, Liz Willner accused them of misrepresenting both VAERS and OpenVAERS. She cited data collected between 1990 – 2010 to argue, misleadingly, that “83% of reports are health care workers and Pharma”. Despite all evidence pointing to her, she insists OpenVAERS is a team effort. This is reflected on the site.
From the FAQ. Why is OpenVAERS necessary?
We built openVAERS because we found the HHS site difficult to navigate and get information from. We wanted a way to browse reports. Once we had that we decided to make it public.
How generous. Who is behind OpenVAERS?
OpenVAERS is a project developed by a small team of people with vaccine injuries or have children with vaccine injuries. We do not accept donations or solicit fees. There is zero monetization of this site. It is purely created in order to help others browse the VAERS records and to identify the reported signals that may otherwise get missed.
Here Willner misuses the term “signals”, specifically in how they relate to establishing risk. According to the CDC under How VAERS works:
Patterns of adverse events, or an unusually high number of adverse events reported after a particular vaccine, are called “signals.” If a signal is identified through VAERS, scientists may conduct further studies to find out if the signal represents an actual risk.
The design of OpenVAERS allows immediate access to VAERS reports. These, in conjunction with tabulated figures, can be easily screenshot and spread via social media. Misleading commentary on these platforms aims to encourage vaccine hesitancy. One claim is that COVID-19 vaccines cause serious cardiac events and heart attack. In addressing this topic the indefatigable Orac picks apart flawed manipulation of data from Robert F. Kennedy Jr. and Children’s Health Defense. Back in May the energetic David Gorski addressed the “vaccine holocaust” based on VAERS data that Mike Adams bravely announced. Examples abound. The one constant, and undoubtedly something to be factored into public education, is that misuse of unverified reports is a key driver of vaccine hesitancy.
Despite long standing problems, VAERS works. RotaShield is a case in point. Twenty years of research preceded its approval by the FDA. Four months after ACIP recommended a three dose schedule for all infants it was suspended to allow for a CDC investigation. There had been twelve reports to VAERS of intussusception. Dorit Reiss, a law professor at UC Hastings and pro-vaccination activist, shares Paul Offit’s view that submitting reports to VAERS should be easy for members of the public. Reiss has suggested withholding reports that are “clearly not credible”.
One imagines this would include suicides, drownings, car accidents, homicides, and so on. To appreciate the less credible, or in this case incredible, consider the case of James Laidler M.D. He submitted a report to the effect that the influenza vaccine turned him into The Incredible Hulk. It was accepted. To reinforce this flaw Kevin Leitch of Left Brain Right Brain, submitted a report to VAERS that his daughter had turned into Wonder Woman following vaccination. This too was accepted. The ease of submitting dubious reports has been raised with antivaxxers. The unanimous reply is that submitting a false report to VAERS is a felony. This was also argued by Liz Willner when defending her conduct to Logically. The Hulk and Wonder Woman however, remain felony free.
It is clear though, that VAERS as it presently exists is of benefit to U.S. public health. Given that so much of the anti-vaccination response to the COVID-19 vaccine rollout was anticipated it is unfortunate that the abuse of VAERS was not proactively met. The outlay of resources to say, educate, or at least inform the public would not be prohibitive. The probable cost of managing the harm that exploitation of the system has, and will continue to cause is significant. Of course that’s an easy observation to make in hindsight. Nonetheless, any measures taken now to manage misinformation adversely effecting vaccine uptake would likely be justified.
VAERS Underreporting
The misuse of VAERS data is rarely complete without also misrepresenting the fact that adverse events following vaccination go largely unreported. In other words VAERS data represents underreporting. Given that the majority of events are minor, such as injection site soreness and redness or involve headaches, fever, aches, nausea, itching and so on, this is to be expected. For the anti-vaccination lobby the aim has always been to create the illusion of large scale death and serious injury, then compound this by claiming it represents only a small fraction of actual cases. Judy Wilyman favoured this tactic to smear successful HPV immunisation campaigns and indeed all vaccines. Liz Willner doesn’t disappoint.
VAERS is the Vaccine Adverse Event Reporting System put in place in 1990. It is a voluntary reporting system that has been estimated to account for only 1% (see the Lazarus Report) of vaccine injuries. OpenVAERS is built from the HHS data available for download at vaers.hhs.gov.
From the OpenVAERS blog post of 2 August 2021:
The 518,769 injury reports are just the tip of the iceberg as a government-funded study concluded that “fewer than 1% of vaccine adverse events are reported.”
This is more decontextualisation. It is unlikely visitors will read the report or indeed search for definitive reviews of the one percent finding. Also, as data are from a government authority, and underreporting is represented on government sites, an appeal to authority is in constant play. Antivaxxers have thus quite confidently used this two pronged approach for over a decade. Adapting to the rollout of the COVID-19 vaccine while obfuscating increased reporting of symptoms and the role of V-Link, has proven seamless for established lobbyists.
The figure of 1% comes from a report from Harvard Pilgrim Health Care, Inc., authored by Ross Lazarus. Data examined are from 1 December 2007 to 30 September 2010. These data include all possible adverse events. Prior evaluation of the reporting rates of various events confirms that minor events are rarely reported and more serious events routinely reported. A 2014 report on surveillance of adverse events following immunisation in NSW, Australia noted that:
Only 11% of the reported adverse events were categorised as serious
Reuters report the case of an antivaxxer reiterating falsely that only one percent of deaths and injuries following the COVID-19 vaccine are reported. The article includes this comment from a CDC spokesperson:
Mild events, like a rash, tend to be reported less frequently than severe events (like a seizure). We have data to show that serious adverse events that occur after vaccination are more likely to be reported than non-serious adverse events. Events such as a sore arm at the injection site might not get reported since they are expected and therefore people don’t feel the need to report them.
A December 1995 study of passive surveillance sensitivity in The American Journal of Public Health reported 72% for poliomyelitis after the oral polio vaccine and less than 1% for rash and thrombocytopenia after MMR. A 2020 study of VAERS sensitivity published in Vaccine noted in Background, a similar rate of 68% capture for poliomyelitis after oral polio vaccine and 47% capture of intussusception cases after rotavirus vaccine. The target objective of anaphylaxis and GBS following various vaccines revealed a range from 12% to 76%. As early as 2003 a study found that serious events are rare.
What antivaxxers won’t tell you
The evident paucity inherent in the misuse of VAERS data becomes apparent when examining another appeal to authority employed by antivaxxers. Namely the amount of money awarded to “victims of vaccine injury” via the Vaccine Injury Compensation Program (VICP). Total compensation paid out over the life of the VICP, since 1988, is in the area of $4.6 billion US. Members of the anti-vaccine lobby often cite various approximations of this figure to underscore their claim that vaccine damage occurs on a huge scale. In fact a simple analysis of VICP figures reveals the opposite to be true.
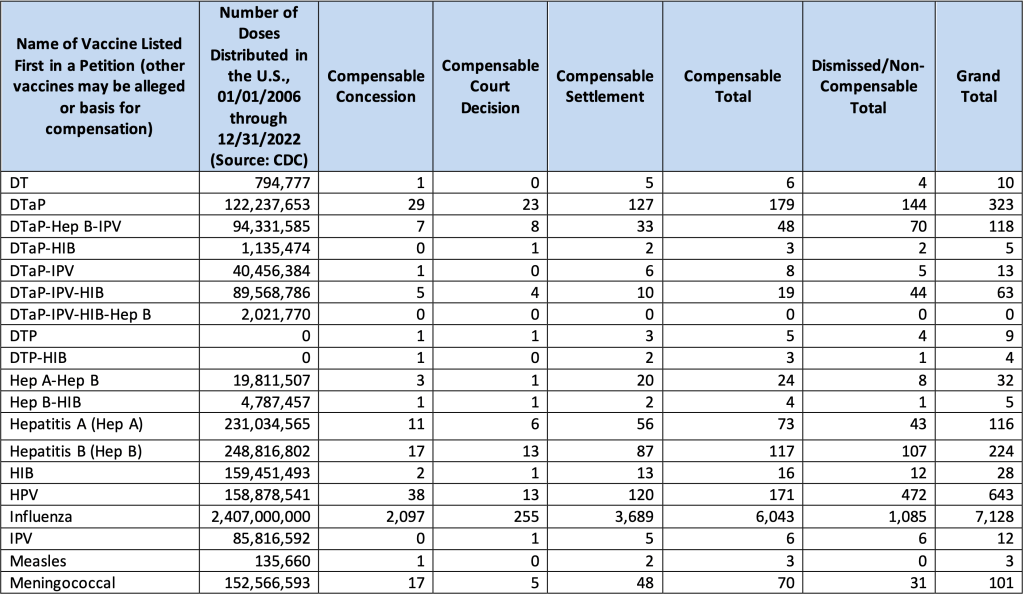
The report states that for every 1 million vaccine doses, “approximately 1 individual was compensated”. This is a familiar figure. The table below contains the monthly VICP statistics update report for 1 January 2024. It may be found on page three of the data and adjudication statistics report from Health Resources and Services Administration. It is headed Adjudication Categories, by Alleged Vaccine for Petitions Filed Since the Inclusion of Influenza as an Eligible Vaccine for Filings. NB: Influenza doses = 45% of total doses since 2006.
From 1 January 2006 to 1 January 2024 the number of vaccine doses distributed, as sourced from the CDC, totals 5,050,074,788. The total number of compensable cases is 8,182. Or 0.00016% of distributed doses. The Influenza vaccine accounts for 73.9% of compensable doses. Total settlements, including dismissed cases and non-compensable cases to date, have reached 11,421. Or 0.00023% of distributed doses. This represents a striking absence of vaccine injury. Unsurprisingly you will not hear these figures from the anti-vaccination lobby.
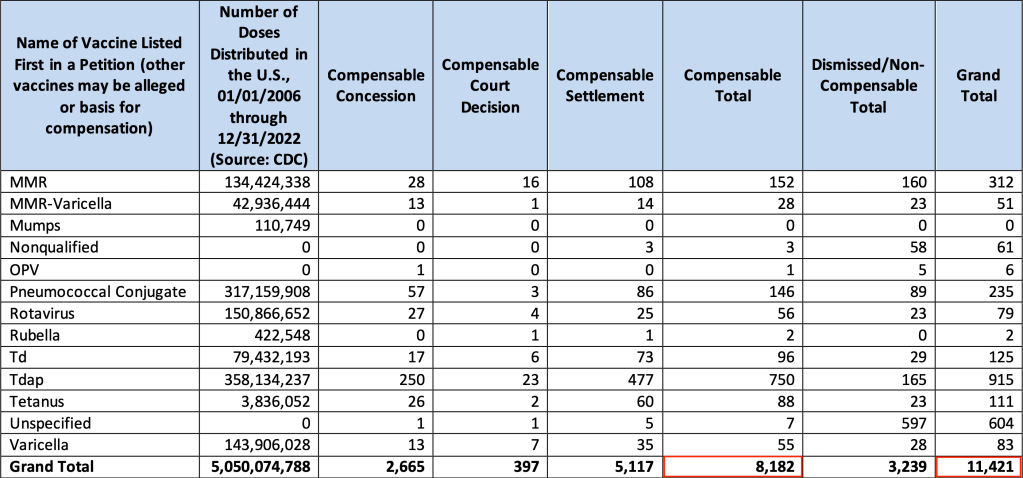
Since January 1988, 24,538 petitions have been filed [page 5]. 8,439 or 34% of petitions were compensated. More so, as the HRSA report states, “Being awarded compensation for a petition does not necessarily mean that the vaccine caused the alleged injury”.
And:
Approximately 60 percent of all compensation awarded by the VICP comes as a result of a negotiated settlement between the parties in which HHS has not concluded, based upon review of the evidence, that the alleged vaccine(s) caused the alleged injury.
Before moving on it’s worth reflecting on the fact that both VAERS and the VICP exist thanks to the efforts of established anti-vaccine campaigners such as Barbara Loe Fisher. Their campaigning led to the creation of the 1986 National Childhood Vaccine Injury Act, which is itself the subject of Andrew Wakefield’s most recent film claiming widespread vaccine injury. As we can plainly see not only are compensated cases exceedingly rare, but only 40% of those demonstrate a causal link to any vaccine. One expects it is not rash to expect that in time we will see similar figures pertaining to COVID-19 vaccines.
Antivax Winning Formula
Misrepresenting VAERS data is a simple winning formula for antivaxxers. It follows that it can be applied to any adverse event reporting system, particularly those employing passive surveillance. The COVID-19 vaccine rollout is unprecedented and subject to significant scrutiny. Governments support the reporting of adverse events and deaths post COVID-19 vaccination. The winning formula thus ensures the anti-vaccination lobby has a significant advantage in spreading its message. Data from the U.K., the E.U. and Australia have also been misused this way. The exploitation of coincidental deaths following COVID-19 vaccination was met quickly and comprehensively by Australia’s Therapeutic Goods Administration. Not surprisingly this had no effect on those opposed to vaccination against COVID-19.
Analysis of application of the winning formula to other government reporting systems is beyond the scope of this post. However, Australians have made good use of the tactic both before and during the COVID-19 pandemic. Underreporting of adverse events was mentioned in a May 2019 press release from the Informed Medical Options Party. They promise a “more accurate” system if elected. More recently, misused data from the U.K. Yellow Card voluntary reporting system was retweeted by Australian senator Malcom Roberts. United Australia Party leader, Craig Kelly, randomly texts Australians with a link to screenshots of reports to the TGA Database of Adverse Event Notifications. In April 2021 Judy Wilyman cited conspiracy theory website accounts of unverified reports to smear COVID-19 vaccine. A flyer packed with false and unverified deaths and injuries from four different reporting systems was tweeted by Meryl Dorey in mid June 2021. Watch this space.
Conclusion
The U.S. Vaccine Adverse Event Reporting System (VAERS) is a passive reporting system open to the public that has, since its inception, been exploited by the anti-vaccination lobby. The absence of any causal relationship between vaccine and report is ignored by antivaxxers. The introduction of the COVID-19 vaccine has accompanied unprecedented reporting due to increased vaccination with active encouragement of recipients to use the VAERS system. The rise in reports was to be expected. This clinical reality has been obfuscated by players in the anti-vaccination community who have skilfully used social media to present background mortality and morbidity as causally linked to COVID-19 vaccination.
The website OpenVAERS, dedicated to misrepresenting VAERS data has focused exclusively on COVID-19 vaccination since January 2021. An investigation by Logically found Lizabeth Pearl Willner from California is the force behind the site. A frenetic antivaxxer, Liz Willner attempted to dismiss her activity as provision of easy access to data. Since the investigation she has been actively removing her anti-vaccination footprint on social media whilst keeping the site active.
Payouts from the Vaccine Injury Compensation Program to date total $4.6 billion. Often cited by antivaxxers as further evidence of widespread vaccine related harm, VICP settlements from 2006 – 2019 equate to 0.00015% of vaccine doses given in that period. The Influenza vaccine accounts for 71.6% of this total.
Misrepresenting VAERS data to convince others that vaccines cause significant harm has proven to be both durable and successful. Combined with the misleading claim that only one percent of all events are reported, the result has almost certainly been an as yet unknown increase in vaccine hesitancy. Familiarising the public with the manner in which such data are misused may alleviate some amount of vaccine hesitancy.
COVID-19 vaccines are safe and effective.
References and reading
Vaccine Adverse Event Reporting System – HHS
Guide to interpreting VAERS data – HHS
Surveillance for Adverse Events Following Immunization Using VAERS – CDC
Selected Adverse Events Reported After COVID-19 Vaccination – CDC
Anti-vaccine activists use a government database to scare the public – Science
Anti-Vaxxers Misuse Federal Data to Falsely Claim COVID Vaccines Are Dangerous – VICE
California Woman Behind Antivax Site Outperforming Government Database – Logically
The Woman Who Secretly Runs One of the World’s Biggest Anti-Vax Websites From Her House – VICE
Hugely Popular Antivax Site Is Just Some Lady In Piedmont
Unverified reports of vaccine side effects in VAERS aren’t the smoking guns portrayed by right-wing media outlets – they can offer insight into vaccine hesitancy – The Conversation
Reports of adverse effects in US database aren’t confirmed to be linked to vaccination – Fact check
Large real-world study: Pfizer’s COVID vaccine is safe
Electronic Support for Public Health–Vaccine Adverse Event Reporting System (ESP:VAERS) – PDF
Underreporting and Post-Vaccine Deaths in VAERS Explained
The reporting sensitivity of VAERS for anaphylaxis and for Guillain-Barré syndrome
VICP Monthly Statistics Report October 2021
VICP Monthly Statistics Report November 2021
Last update: 27 January 2024
♠︎ ♠︎ ♠︎ ♠︎

Pingback: OpenDAEN: Misleading Australians | Losing In The Lucky Country
Pingback: Turbo Cancer: Time for this anti-vaccine myth to die | Losing In The Lucky Country