
In June this year we briefly met suspended GP registrar, William Bay, thanks to his attempt to intervene in the Australian Babies Case. He has summarised his reasons for doing so here. Suffice it to say the Australian Vaccination-risks Network were not happy, making me very happy.
Fast forward to the present, and former AVN president Meryl Dorey, who has taken to feverish promotion of cooker-conspiracy theories on Substack, revealed Saturday that the same William Bay had sent her a formal Letter of Concern. It lists numerous comments about him on her Substack site, that he believes are defamatory. Billy wants the article and every comment removed, topped off with a public apology. This is the latest event since Billy, who proudly refers to himself as the Suspended Dr. William Bay, falsely declared his High Court challenge to have the Voice referendum declared unconstitutional, was a success.
This was not the first time Billy, who often proclaims he’s doing God’s work, declared victory in stark dissonance to the facts. He is soundly refuted by AAP FactCheck here. AAP provide insight into how quickly disinformation spreads between cookers. Billy’s proclamation of victory is a great example of how the uncritical acceptance of a claim can influence belief. It also underscores the power of social media, in this regard. Billy gave a performance of confidence and credibility in a Cafe Locked Out interview, citing as proof documents that actually confirmed his failure.
During the interview he referred to a document on his website’s legal docs page headed “Application For A Constitutional Or Other Writ”. Billy directs viewers to his site then says:
I’m looking at it on my computer right now. It’s a miracle, it’s gorgeous, it’s great. It is a stamped document by Justice Jagot of the High Court itself who has declined to rule on the constitutionality of the referendum. So with this case being dismissed from further need for analysis, in legal circles as my lawyer friends will know… if jurisdiction is not proven it is invalid.
The gorgeous and great miracle was the exact document Billy had submitted for filing. The stamp added by Justice Margaret Jagot references High Court Rule 6.07.2, which deals with the management of frivolous or vexatious applications, and includes:
I direct the Registrar to refuse to issue or file this document without the leave of a Justice first had and obtained by the party seeking to issue or file it.
The upper part of the stamped application is below.

Screenshot – Billy Bay’s rejected application
Of course I am not a lawyer, and neither is Billy for that matter, but he has filed documents with the High Court before this. The Notice Of Filing cover page is part of previous documents he has lodged, displayed on his website. This includes file number, title, registry, type of document; in this case Application for constitutional or other writ, filing party and date. Think of it as confirmation that legal proceedings will take place. Plainly absent from his gorgeous miracle, it also clearly states:

Notice of filing page: Important Information
Staying in theme dear reader, I submit that the evidence before you supports the contention that the Suspended Dr. William Bay did know or should have known that his application was unsuccessful, and did know or should have known that the 2023 referendum is not unconstitutional. This conduct is not unusual for Billy who frequently offers baseless beliefs as fact.
Nonetheless, what followed was an old fashioned pile-on by various “freedom fighters” who took three days and more to decide Billy was wrong. Which interestingly, although they’d never admit it, was how long it took for AAP FactCheck to publish their rebuttal. More so, the stamped rejection of Billy’s application was available on 5 September receiving comment on social media by critics of the so-called freedom movement.
Then on 8 September, long time anti-vaxxer, AVN member, self-proclaimed “journalist” and founder of The People’s Revolution, Tristan Van Rye, better known as Triccy Triddy took to Facebook. Triccy lives in that alternate universe where nefarious global conspiracies of momentous proportion are accepted as fact. His tactics deserve proper deconstruction, but for now bear in mind he is driven by base neoconservatism. There is the ever-changing enemy to fear and there is “us”, constantly threatened by the enemy. Triccy’s a true believer and whilst he’s sowing fear, disinformation and social harm, appears genuinely convinced he is doing good.
In this video Triccy does a sound job of pointing out why Billy’s claim that the referendum is unconstitutional, can only be bogus. Chatter in the cookerverse following Billy’s announcement was reinforcing his other claim, that voting is unnecessary. Triccy had spent months sewing disinformation and anxiety about voting “Yes” and understandably couldn’t allow the chance of lost votes to go unchallenged. Other seasoned curators of disinformation felt the same way and rushed to their live streams. Senator Malcolm Roberts (who himself alleged in parliament that the ballot was unconstitutional), AVN president Aneeta Hafemeister, SovCit grifter Mike Palmer, former MMA fighter and Peacemaker founder Nick Patterson and pseudolaw obsessive Derek Balogh, all had a sudden concern for the spread of misinformation.
In the wake of Triccy’s video, Billy sent him a text message. It was reposted on Telegram:
Triccy, I hearby request and direct you to take down that FB live that you just did about me because I consider it defamatory.
We have WON in the High Court. I will continue to show and explain that to the people of Australia; until it’s crystal clear for everyone I encourage you to keep an open mind to things, and in the meantime, I would appreciate it to save us all the trouble if you would remove that video please. Dr William Bay
Then suddenly:
Billy also sent a Letter of Concern to Triccy in response to said defamatory video. Triccy, in a rare moment of near jocularity, burnt it in his favourite faux lounge fire-pit. Billy however, kept up his booming confidence and applied for leave to issue or file the original application. This matter was heard on 15 September and ruled the original application an abuse of process. See p. 5, para 8:
It is not necessary to consider the question of standing, here in the context of a referendum. By r 6.07.1 leave to issue or file should be refused where the document would amount to an abuse of process. The latter term encompasses proceedings which are foredoomed to fail, as the proposed proceedings are.
Ah, foredoomed to failure, dear reader. A weighty yoke for our suspended doctor to bear. By 19 September, Billy had apologised to Triccy and withdrawn “proceedings”. Triccy was not amused, and announced an end to any further cooperation with Billy. He also took issue with a claim Billy made about employment restrictions imposed by AHPRA. We’ll get to that. First, we don’t want to forget that when Billy was gearing up to sue Triccy for defamation, someone else got their bad ass boots on. In fact there was bad assin’ and chin juttin’ aplenty from our Meryl, all with the hope of provoking Billy.
He was easy to provoke and Meryl went in hard. In a piece titled Distinguishing truth from bullsh*t 101, Meryl hit him where it hurt. It began with humour, as Australia’s most pernicious antivax liar laid out the section heading; Unity is vital – but truth is paramount. Oh, how we laughed! But next came mockery with; Billy Bay’s High Court “Victory”. Ah, the sting of those quotation marks. Then Not the first time Billy has done this, opened the way to a recounting of the failure of the Australian Babies Case. But ultimately came the totally bad ass; Will Billy Bay now come after me for telling the truth about his actions?
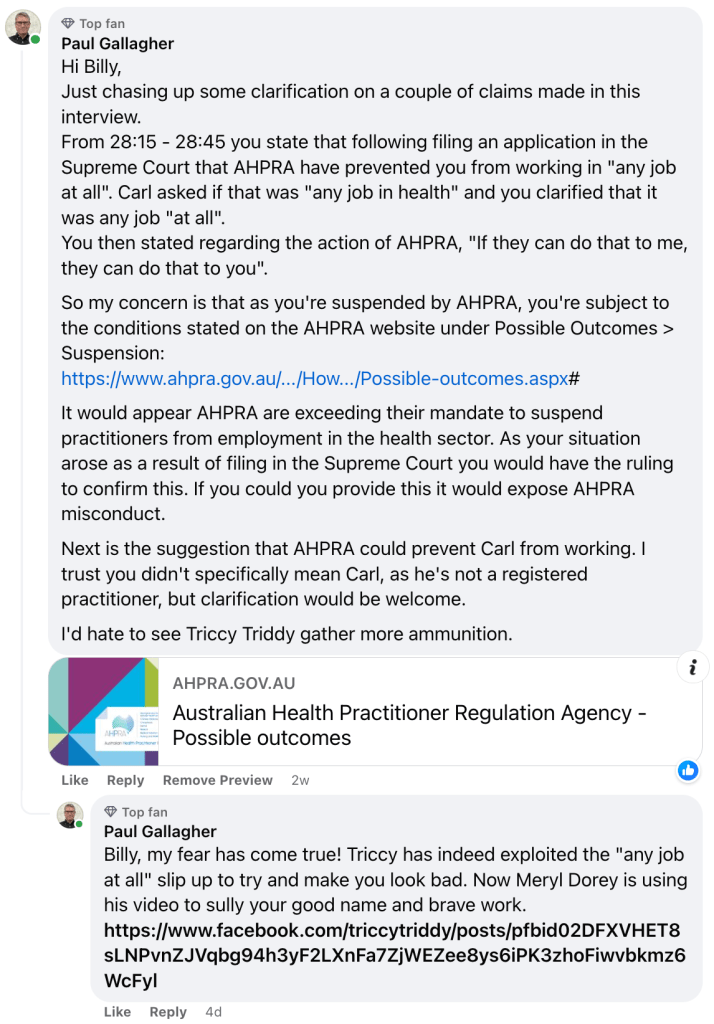
Having got the desired reaction, Meryl posted an article, referring to him only as “Bully” as she outlined the specifics of Billy’s letter of concern. The subheading; I don’t take well to threats, can only be described as (need I say it?) totally bad ass, and the article swiftly dispenses with any notion that Meryl is concerned. Within, she refers to a comment reply she wrote in response to Billy’s comment requesting her to “stop attacking” him. She raises the same issue Triccy Triddy had done regarding Billy’s claim on Voice of Freedom that AHPRA had prevented him from working in “any job at all”.
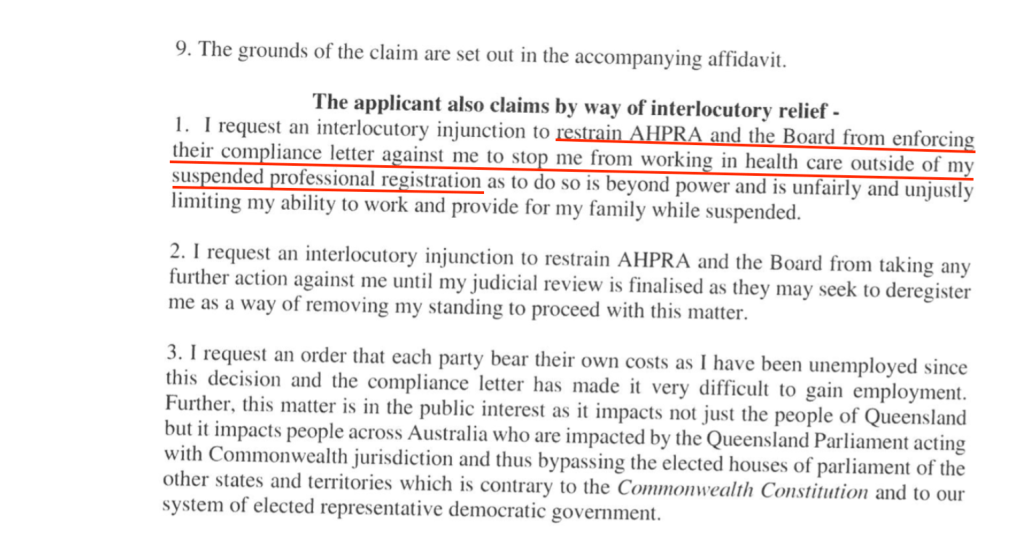
This is another jolly example of that area between remote possibility and reality that Billy exploits. Just as he continued to claim victory in the High Court because he had filed for leave to have his (already rejected) application accepted, there is a submission Billy refers to in the hope of convincing his followers. Simply put it is material submitted in reply from Billy to AHPRA, The Medical Board of Australia and QLD State, in the wake of his suspension. It happens to include:

So, he sought an injunction to prevent AHPRA and the Board from further enforcement of their “compliance letter” so that he can work in positions that don’t “require current registration with AHPRA as a condition of employment”. Neither AHPRA nor the Board have the power to enforce conditions outside their purview. Billy has always been free to work in areas where registration with AHPRA is not required.
Prior to this Billy had submitted an Application for Review of the findings of AHPRA and the Board. On page 7 is a request for an injunction to limit enforcement of the “compliance letter”, so that Billy could work in health care roles seperate from those of a GP Registrar.
The “compliance letter” is clear in that Billy is prohibited from working in health care. All health care, and only health care. In fact, the same document includes a November 2022 affidavit from Billy Bay which presents a clear summary of that letter on page 4, item 15:

The evidence that AHPRA ever sought to prevent Billy working “at all” doesn’t exist. Yet Billy chose to zero in on one part of a much larger, failed application to the Supreme Court. From 27:20 to 28:45 in the interview with Carl Lieberman, Billy talks about what he then thought were defamatory comments from Triccy Triddy. It was “a matter of life and death” for him because if his followers don’t trust him, donations would dry up and this was his only income. You can grab the mp3 file here or listen below. The important part is:
Billy: I even filed an application in the Supreme Court to let me work in any job at all and I lost that one…
Carl: Is that any job in health or any job at all?
Billy: At all, at all Sir… at all! It’s an outrage. It’s a disgrace and a disgust and the people of Australia need to know that, to see how unlawful this AHPRA agency is that they think they can regulate me that much. If they can do that to me they can do that to you.
Carl’s face is priceless as he can’t hide his incredulity. He asks Billy about responding to AHPRA under basic trade-law rights, but Billy had already tried “the international covenant on political and civil rights”. And so it came to pass that Triccy and Meryl called foul on this claim of Billy’s. But they were ten and fourteen days late respectively. Where did they get such bad ass information? Could it be that badder asses had earlier sought to hold Billy to account? A quick visit to Billy’s Facebook page gave me an answer of sorts. Some devious character with an obviously fake name had commented under the video, a day after it was posted:
The plot thickens! There’s also some lucky losing cast iron flying pig standing on an old copy of The Skeptic magazine and snooping around X.
Humour aside, there are serious elements to consider in the wake of Billy’s ultimately harmless threats against seasoned con-artists. It’s breath-taking to witness Meryl Dorey, architect of the 2016 No Jab No Pay High Court scam, levelling accusations of donation fraud against him. NSW Fair Trading found the AVN guilty of breaching the Charitable Fundraising Act 1991, yet decided not to press charges. As for the money Dorey admitted to hoarding, furious AVN donors had to swallow the loss of their $160,000. Yet she recently wrote about Billy:
So Bully is gaining money from our suffering community under false pretences and I exposed that along with several other long-time supporters of health freedom and informed choice.
Meryl exposed nothing others hadn’t revealed two weeks before. Her own false pretences ensured a career sabotaging public health initiatives and scamming donors. Prior to the formation of the unfunded volunteer group, Stop The AVN, her unceasing schemes ran unchecked. COVID was a double-edged sword; bringing more followers to anti-vaccine conspiracies, but ensuring the increasing irrelevance of the Cult of Meryl. Even the AVN court cases failed. The frustration seeps through in this stand-over advice she offered Billy.
Better than you have tried to censor me for nearly 3 decades and they have not been successful. Perhaps it’s time for you to do some deep soul searching Bully and try to work out why you are actually involved with this issue. Because as far as I can see, it doesn’t appear that caring for our community and the lives of the children and adults therein is your main motivator.
Triccy was far more diplomatic in his criticism, stressing that he meant Billy “no harm”. Unlike Dorey, Triccy appears genuinely focused on change rather than profit and ego. That said, his belief that “we are experiencing World War III, which will be known in the future as The War Against the People”, is based on harmful conspiracy theories of shadow governments. Whilst a key aspect of his rhetoric is that “people will forget their differences”, he is quite skilled at ensuring division between what he wants and what most of us identify as progressive thought.
Billy himself has spent over a year filing for court cases, circling social media and attending protests, after he publicly sabotaged his medical career at an AMA conference in July 2022. Like these other two judging him, he spends a great deal of time spreading disinformation to suit his own bizarre ideology. He also scoops up donations from gullible supporters drawn to conspiracies.
Ultimately, trouble in cooker paradise is nothing short of great news. Belief in conspiracy theories and suspicion of vaccines have both increased post COVID. Researchers are refining their understanding of the factors behind distrust of health authorities. Yet the role social media played in warping uncritical minds during lockdown, has today been replaced by quick-changing narratives adapted to suit. Attacking the Voice referendum is a case in point.
For a long time yet, anything that reflects positive social change will be seen by these players as the latest phase of dark conspiracies. I for one wish them all the infighting and trouble they can muster, and may they tear their angry little worlds asunder.











