The Medical Board of Australia has placed fifteen limitations on the practice of Dr. Stuart Reece of Highgate Hill QLD. The conditions, enforced on 21 December 2022, have resulted in the temporary closure of the Southcity Medical Centre where Reece practices.
Reece (pictured) is a controversial figure in addiction medicine and a vocal critic of Australia’s successful policy of harm minimisation. He holds no formal qualifications in addiction medicine, but has authored or coauthored extensively on the subject, presently as an adjunct professor at UWA. Almost exclusively, his writings link illicit drug use, methadone and medical cannabis to death and disease.
Experts have refuted certain works as “reefer madness”. Reece has long associated his Christian faith with treating addiction. His book, titled “Let My People Go: A Theology of Addiction”, was published in 2016. His work is favoured by extreme anti-drug pressure group, Drug Free Australia, and frequently cited by them in lobbyist material, media replies and parliamentary submissions.
This is not the first time regulators have acted to ensure the safety of his patients. An article published on this blog in December 2011 examined his use of unapproved naltrexone implants and the deaths of 25 patients who had undergone the treatment. In 2009 Reece was suspended from practice for supplying morphine to opiate dependent patients and falsifying records to disguise the fact. This was because of his ideological opposition to evidence backed methadone maintenance therapy. That suspension was in turn suspended for three years.
The Medical Board of QLD, Health Practitioners Tribunal observed at the time that Reece:
… has a somewhat evangelical approach to this area of medicine and because of that he does appear to lack a degree of insight and objectivity in relation to the treatment of his patients. Furthermore, he seems to feel that the ends justify the means in terms of treatment of patients.
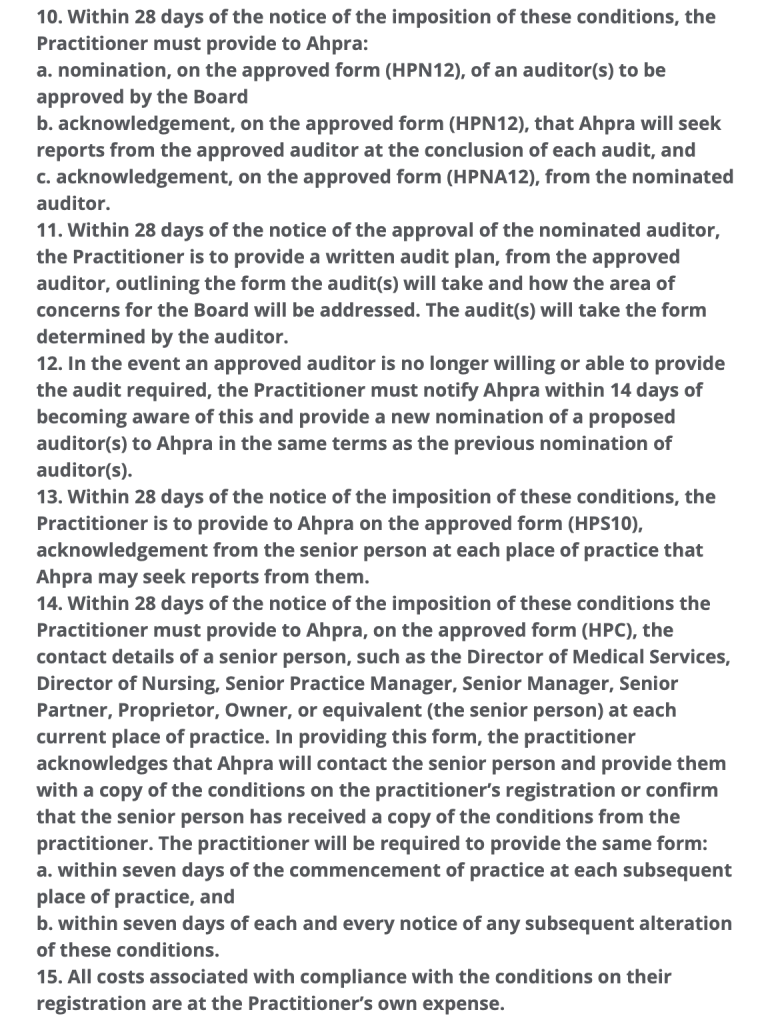
Today, the catalyst for intervention includes the number of patients being bulk billed per hour and quality of care. This is reflected in the limitations on practice (complete list in slideshow below).
1. The Practitioner must not exceed four (4) of patient consultations in any one hour (60 minutes). […]
5. The Practitioner must only practise as a general practitioner when supervised by another registered medical practitioner with knowledge and experience in addiction medicine (the supervisor). For the purposes of this condition, ‘supervised’ is defined as: The Practitioner must consult with the supervisor who is always physically present in the workplace and available to observe and discuss the management of patients and/or performance of the Practitioner when necessary and otherwise at weekly intervals. […]
7. In the event that no approved supervisor is willing or able to provide the supervision required the Practitioner must cease practice immediately and must not resume practice until a new supervisor has been nominated by the Practitioner and approved by the Board.
A search for general practitioners providing services in addiction medicine in the Brisbane area yields modest results. There just isn’t enough practitioners providing these select services across Australia. If one adds the fact that such providers have often taken on all the patients they can, it isn’t beyond comprehension that Dr. Reece is unable to find a supervisor. Reece has loyal supporters amongst his patients, who have a Facebook page here. They have argued in a petition that finding a supervisor is “an impossibility”. The petition, “Reinstate Dr. Stuart Reece Immediately”, contends that the predictable lack of a supervisor indicates that the action taken is about the control of services offered under bulk billing.
AHPRA is also advising that Dr Reece must have another Doctor with him for consultations into the future to oversee his work to their satisfaction. This requirement is an impossibility. AHPRA and Dr Reece both know that this doctor does not exist. There is not a ‘spare doctor’ lying around that is available for this. […]
THIS IS NOT ABOUT PATIENT CARE OR BETTER HEALTH OUTCOMES. THIS APPEARS TO BE ABOUT CONTROL OF THE TYPE OF SERVICES OFFERED TO PATIENTS WHO NEED BULK BILLED DOCTORS.
The petition is a long heartfelt plea seeking to justify the way Reece operates his practice. It makes the point that certain appointments, particularly prescription refills, may require only five minutes. The petition also notes that Reece would be forced to close his doors in part because, “his practice would be limited dramatically by the immediate reduction of the number of patients he is able to see daily…”. Whilst I empathise greatly with these patients and find removal of any addiction treatment services troubling, one cannot escape the fact that such a huge patient load should never have eventuated. Health Practitioner Regulations state, “A Practitioner must NOT exceed four (4) patient consultations in any one hour (60 minutes)”.
There’s no doubt that Medicare is not meeting the needs of Australian General Practitioners. The patient rebate is beyond inadequate, being markedly out of step with the Consumer Price Index (CPI). This manifests in significantly fewer consultations being bulk billed, and in many practices fees now apply to concession card holders. For Australians surviving on the aged or disability support pensions a visit to their GP is now financially prohibitive. The end result is a health system under strain. However there comes a point where increased patient quantity, means decreased quality of care. Let’s remember that the Health Practitioners Tribunal observed in 2009 that when it came to treating patients Reece lacked insight and objectivity, and felt the ends justified the means. The same document notes (point 22):
He does provide care to a large number of detoxifying and drug dependent patients. In June 2009, alone, he had 409 Subutex patients in Queensland and I understand the numbers are larger at the moment. From 2001 to 2007 he was responsible for 8681 registrations of opiate withdrawal registrations in Queensland.
Arguably, Reece is the architect of his own professional distress. As noted above, in November 2009 the practice suspension applied to Reece was itself suspended for three years. Yet less than two years later there was no tone of contrition for falsifying medical records to supply opioid dependent patients with morphine. The occasion was a Senate Inquiry into the Professional Services Review (PSR) Scheme, to which Reece, representing the now defunct Australian Doctors Union, made a submission. Bear in mind Reece has today been saddled with limitations to prevent excessive bulk billing at the expense of Medicare. The PSR “aims to protect the Australian public from the risks and costs associated with inappropriate practice within Medicare…”. Reece began his submission:
Prof. Reece: The Australian Doctors Union is a nascent union which has come together to support each other through the nightmare experience of PSR’s incompetence, lies, intimidation and bullying. In addition to doctors damaged by—
CHAIR: Hang on please. That is making accusations and it is not the way that we take evidence. If you could please refrain from using that sort of language, that would be appreciated.
Reece continued for a full five minutes explaining why he believes the PSR “has been shown to be waging a very successful war against general practice in this country”. He blamed the PSR for doctor suicides, marriage breakdowns, a lowered bulk billing rate, marginalisation of women, being racist, sexist and for damaging “many excellent doctors”. One of these was his ideological colleague, “Dr George O’Neil of naltrexone implant and detox fame”. Despite the fact naltrexone implants are not TGA approved Reece felt O’Neil should have been assisted by Medicare. Perhaps most alarming was when Reece included himself as one of those excellent doctors. Referring to himself in the third person, he humbly submitted:
Associate Professor Stuart Reece, one of the foremost detox doctors in the nation and a world authority on the long-term effects of opiate addiction.
This dear reader, is the crux of the matter. Stuart Reece is not a world authority on the long term effects of opiate addiction. In 2007 he opposed needle-syringe programmes, methadone maintenance therapy and the policy of harm minimisation in general. He informed a parliamentary inquiry that condom use was linked to AIDS deaths. Yet in June 2009 Reece was managing 409 Subutex patients. Buprenorphine is the opioid in Subutex and today it is distributed in combination with naloxone under the brand name Suboxone. It is a successful mainstay of substitution therapy for opioid dependent patients seeking to manage addiction and eventually cease opioid use. It is a key element of harm minimisation.
Exactly how a strident opponent of harm minimisation has today found himself with so many opioid substitution patients that Ahpra require supervision and auditing of him, is baffling. It may however have something to do with the attitude toward Medicare and the PSR Scheme reflected in his 2009 submission. Or his 2012 comment, What is wrong with medicare? (p. 170) bemoaning the PSR and Medicare audits. It may also have something to do with the disdain Reece has for evidence based health policy and genuine, original research. Reece has spent a career convinced he simply knows better. Better than the bulk of his colleagues, better than global research trends and better than health authorities. In short, Stuart Reece is the cause of the dilemma faced by so many of his patients.
Having said that, one cannot deny that Reece and Southcity Medical Centre have been accomodating the needs of a great many patients. An excessive number of patients. However accounts such as this on reddit aren’t isolated. They suggest the practice is busy, waiting times are high but Reece is attentive and compassionate. Google reviews are more varied. According to the petition there are 1100 patients in need of treatment. Over the last 18 days, 224 people have signed. The goal is presently 500.
Ultimately this situation doesn’t bode well for these patients. It is doubly sad that many are not able to see that the cause of their problem is Stuart Reece himself and not Ahpra. Funnelling high numbers of vulnerable in-need, at-risk patients through the surgery is far from acceptable. The only way forward is to abide by the limitations. Anything less is to abandon his patients.
Stuart Reece must accept that the ends do not justify the means. It is time to place patients first.
Medical Board of Australia restrictions imposed on Dr. Stuart Reece
An interesting story sits hidden away in the June 2003 edition of Focus magazine – a QLD based fundamentalist Christian publication.
On page one we meet Graham Preston who was jailed back in June 2003 for pro-life antics. His sole direction was Proverbs 24, verse 11: “Rescue those being led away to death”.
The story on page two is about Drug Free Australia member, Dr. Stuart Reece (below). Thinking of the above proverb, it is disturbing to learn that over a period of twenty months, twenty five opioid dependent patients who sought his care, died following insertion of unregistered naltrexone implants.
Story from Focus QLD June 2003
Naltrexone is an opioid antagonist. In a 2013 position statement on naltrexone implants the Royal Australasian College of Physicians stated on page 6:
The World Health Organisation, UNODC (United Nations Office on Drugs and Crime) and UNAIDS (United Nations Program on AIDs/HIV) have endorsed treatment with methadone and buprenorphine. The World Health Organisation has included methadone and buprenorphine in its Essential Medicines List. Naltrexone has not been endorsed by any United Nations organisations nor is it included on the Essential Medicines List. […] The RACP does not support the routine use of sustained release naltrexone formulations (implants or depot injections) while the product is not registered with the TGA.
In 2003 when the Health Practitioners Tribunal adjourned Reece’s case indefinitely, such implants were available through the TGA Special Access Scheme. This 2008 article posing the question of safety, examines implications of the scheme and difficulty in securing sound data. The authors note:
The strong theoretical rationale for the usefulness of naltrexone in treating heroin dependence justifies further rigorous investigations. However, the uncontrolled use of unregistered products of uncertain quality hampers the development of proper clinical trials.
Above, we read that Reece was “deeply hurt” by the investigation that followed. The families of his dead patients are not considered. Incredibly, the above Focus article claims that the charges brought against Reece were “based on false reports by drug addicts”. No evidence is presented in support of this statement. No independent source has confirmed the existence of false reports. Brought by QLD Health, the charges were just and likely saved lives.
There’s a familiar, yet awkward tactic advanced in his defence. The type of logical fallacy that suggests if positive feedback is presented then to suggest otherwise is not only wrong but “false”. Someone has provided the Focus author with decontextualised data designed to be critical of methadone maintenance therapy. This argument is frequently used by the opponents of harm reduction and proponents of naltrexone. We read “590 patients died with methadone in their system”. It’s an underhanded attempt to suggest methadone was the cause of death. Note this doesn’t read, “died because of methadone overdose or complications”.
We don’t know the cause of death, but I’m certain if methadone was the cause this article would have made it abundantly clear. These figures are pulled from toxicity data in coronial reports. They include hospital patients receiving palliative care, out-patients receiving pain relief, road fatalities, suicides, homicides, poly-drug related deaths and so on. All opioids carry risks and fatalities do occur in the opioid maintenance demographic. Nonetheless, when prescribed by a GP and dispensed in a controlled environment as is the case in treatment of opioid addiction, methadone is a safe option.
I can’t comment much on a reference to a “recently published article” without the source, other than to note that rapid detoxification can pose a significant risk of overdose. Naltrexone has been used orally to block the effects of opioids. The National Drug and Alcohol Research Centre note in, Mortality related to naltrexone in the treatment of opioid dependence: A comparative analysis;
Because naltrexone blocks the actions of opioids, naltrexone rapidly removes a person’s tolerance to opioids so that a given dose of opioids would have more effect than previously. The lack of naltrexone, not its presence, exposes a naltrexone-maintained patient to risk of opioid overdose. If naltrexone treatment is ceased, individuals may be at risk of opioid overdose if they choose to return to opioid use.
Regarding the safety of naltrexone in comparison to the safety of methadone or buprenorphine in the management of opioid addiction, one reads:
When considering deaths per periods of high and low risk, the mortality related to naltrexone was approximately seven times that of methadone during the period of high risk and three times the rate during the period of low risk. […]
This study also found that the mortality related to oral naltrexone treatment was higher than that for buprenorphine and methadone… whether estimated as deaths per 1000 treatment episodes or per 100 person years of risk, the death rate for naltrexone was higher and we believe the estimate provided here is a conservative one. […]
The mortality rates suggest that oral naltrexone treatment, as it is provided in Australia, can place recipients at significant risk of death, and at higher risk than buprenorphine and methadone. However, it should be noted that naltrexone treatment is a useful option in some well-motivated patient subgroups that form a minority of the opioid-dependent population.
Regarding implant technology:
A number of potential issues also relate to this form of treatment, and rigorous research is certainly required to carefully examine the potential for this delivery system to represent a viable treatment option for opioid-dependent persons. Specifically, these issues are: the lack of randomised controlled trial evidence of naltrexone implant efficacy in the treatment of opioid dependence; considerable inter and intra-subject variability in the blood levels of naltrexone resulting from an implant (and so the level of opioid blockade); the lack of good monitoring of adverse events relating to the use of naltrexone implants; and the acceptability of the naltrexone implant preparation to patients and medical professionals.
The article also identified that an existing lack of systematic data reception by coronial databases, hinders accurate assessment of fatalities related to treatment with naltrexone. In 2008 The Medical Journal of Australia elucidated on this problem when it published a paper identifying twelve hospital admissions, related to implants, to two Sydney hospitals over a 12 month period beginning in August 2006. The Abstract conclusion read:
These severe adverse events challenge the notion that naltrexone implants are a safe procedure and suggest a need for careful case selection and clinical management, and for closer regulatory monitoring to protect this marginalised and vulnerable population.
Thus, in attacking methadone as a treatment modality, Reece raises concerns with this author about his impartiality. A read of Dr. Reece’s articles in the arguably biased Journal of Global Drug Policy and Practice is revealing. Also, purporting that methadone causes premature ageing and cell death, without presenting a mechanism and correcting for other variables such as smoking, nutrition and other lifestyle habits is poor science. In the above Focus article this is presented, without a source, as “new research suggests”.
The Focus article was in error to claim vindication. The QLD Health Practitioners Tribunal adjourned indefinitely over the twenty five deaths. It was beyond ambitious for Reece to claim, before a Parliamentary inquiry, to “hold the world safety record” in administering this very treatment. Such comments have little to do with supporting evidence, and more to do with misinformation.
By 1999 research indicated naltrexone was potentially unsafe despite seemingly miraculous stories of recovery. As an opiate blocker, it was emerging with the promise of a quick solution. Yet controlled trials were lacking. Wodak and Hall discussed the evidence in an editorial in the MJA, that also briefly noted the role of the media in confusing community attitudes. Under Parliamentary protection Dr. Reece accused Hall of “scientific fraud”.
In September 1999 the practice of Dr. Stuart Reece was raided following concerns with his approach to addiction treatment. Threatened with closure, he claimed that the QLD government would have blood on itʼs hands if he could not resume practise. Ultimately, he was not closed. Twenty months later, 25 of his patients were dead. ABC 7:30 reported on 4 June 2001.
KERRY O’BRIEN: When the anti-heroin addiction drug Naltrexone was introduced to Australia five years ago, it was hailed as a breakthrough.
Since then, thousands of addicts have been treated with Naltrexone, successfully breaking their deadly habit.
But despite initial expectations it hasn’t proved to be a universal remedy by any means.
Many addicts have lapsed back into heroin abuse and some have subsequently died from overdose.
In Queensland, an investigation is now under way into the practice of Naltrexone activist Dr Stuart Reece, after the deaths of 25 addicts who had undergone his program.
The investigation has already prompted a ban on the use of experimental Naltrexone implants, designed to take the place of tablets.
All had followed the Reece regimen. He was raided by the QLD Medical Board and again closed down. Rev. Fred Nile, speaking as leader of the Christian Democratic Party said at the time:
The action taken by Queensland Health is heavy handed intimidation against those who show true compassion toward heroin addicts. It would appear, by this move, that Queensland Health would prefer that addicts remain addicted to heroin. I fear that this is another step in the mounting campaign for government provided free heroin
Three months later he claimed twenty five “drug addicts” died as “part of a conspiracy”. In September 2003, The ABC featured Reece on their Sunday Nights programme:
Stuart Reece is a Brisbane doctor who finds himself in a bit of bother some of his fellow medico’s at the moment because of his conviction that faith can be instrumental in curing what ails one… The difference perhaps is that Stuart Reece is a born again Christian believer, and makes no apologies for his direct appeal to the Christian Gospel and the power of Christ.
Clearly, the largely untested naltrexone implants were in this case a problem. Had basic support, such as a contact or counselling been available, the recovering patients would have been more safely monitored. It is regrettable that there was undue faith in naltrexone combined with a moral objection to opiate replacement therapy. This is complicated further, in that had naltrexone been demonstrated as effective, financial rewards would have been significant.
In addition, the November 2009 Health Practitioners Tribunal transcript, Medical Board of QLD vs Albert Stuart Reece makes for compelling reading. An unrepentant critic of methadone Reece chose to illegally supply opioid dependent patients with morphine. The transcript includes:
It is clear from his evidence before the Tribunal that he is also very passionate about his practice and in strong disagreement about the continued use of Methadone as a treatment for heroin addiction. […]
Particulars of the referral notice in this matter are that the Registrant on 39 separate occasions supplied Morphine intended for use by drug dependent persons without obtaining approval from the Drugs of Dependence Unit in preparation either for Naltrexone treatment or other detoxification treatment. […]
He admits to doing so and to falsifying medical records when doing so and involving third parties in this conduct. […]
But it is also clear from his evidence, and as I’ve already said that he’s a man who has a somewhat evangelical approach to this area of medicine and because of that he does appear to lack a degree of insight and objectivity in relation to the treatment of his patients. Furthermore, he seems to feel that the ends justify the means in terms of treatment of patients.
In October 2005 Christian conservative MP Tony Abbott Liberal (then Federal Health Minister) funded Drug Free Australia to the tune of $600,000. They did not adhere to conditions under which they were awarded the funding, ultimately emerging as right wing lobbyists. They are followers of Swedenʼs zero tolerance policy and the USA hardliners [open letter]. Reece, a supporter of biblically driven abstinence and a Texas trained fundamentalist, was supported by Drug Free Australia.
By April 2007 Dr. Reece was testifying to the Standing Committee on Health and Human Services (see below) that the immoral policies that permitted condoms – the real cause behind AIDS – clean needles, opioid therapy for addicts, non-punitive cannabis laws, harm reduction and general tolerance for ill Aussies would be our doom. The Senate Standing Committee looked on as Reece introduced himself by saying, “I certainly know the science”. He then displayed a photo of “the archaeological site of Sodom” and a tree with snakes instead of branches. [Page 33/FHS 27]. He explained its relevance. “There will be consequences”.
Reece attempted to explain the moral consequences of policies such as Harm Minimisation, by blaming a tsunami on Divine punishment. He added:
I was interested to discover that the actual historical site of Sodom and Gomorrah has recently been found in Israel. On the bottom right of this slide are pictures of sulphur balls that have been found there. So consequences matter, and they can destroy a civilisation quickly, as we saw with yesterday’s tsunami and so on.
This slide shows a tree with snakes, which to my mind is a lot of the stories that you hear from harm minimisation. Methadone, syringe giveaways, injectingrooms, medical cannabis, heroin trials all those are catered for by the same people. But, on the other side of the tree, you have all the downsides, the side effects, which are not talked about in this culture. It is of extreme concern to me that medical science which is known and understood overseas is not understood and not talked about and given no airplay whatsoever in this culture.
These are old slides I made several years ago, charting a lot of these behaviours: this is condoms and the AIDS risk, charting the parallel between condoms and AIDS deaths.
Ms GEORGE (Senate committee member): Sorry, I do not understand. What are you saying – condom protection andAIDS deaths are correlated?
Dr Reece: Yes, condom sales and AIDS deaths. I am saying that there is a statistical association between the two.
As reported in Crikey by Ray Moynihan Reece decided the “disease drugs, sex and rock-n-roll” was the problem. Asked about the safety of naltrexone, Dr. Reece chose instead to attack internationally renowned scientist, Dr. Alex Wodak [Page 59/FHS54], who specialiseʼs in blood born viruses and epidemiology. Put differently, this means Wodak supports condoms, clean syringe access and used syringe collection: dire threats to our very civilisation, contended Reece. Yet Australian communities with dozens of dispensaries and hundreds of clients report no methadone deaths.
How did Committee Chairperson react to this? Bronwyn Bishop abused public health scientists (who had outlined the success of decriminalisation in Europe), yet she gushed in support of Dr. Reece. A pre-determined agenda in what was billed as the most important family-relevant inquiry of Howardʼs government spoke volumes. Bishop’s final report was rejected nationwide by all but religious fundamentalists and Christian lobbyists. Not one publically funded treatment or advocacy agency missed the opportunity to criticise the report. Bishop went on to call for the removal, and adopting out, of the children of parents struggling with addiction. Should parents conquer their addiction there would be no chance of reunion:
Their [Liberal-led House of Representatives] controversial plan – which also includes compulsory treatment for teenage addicts, restrictions on methadone programs and withdrawing funding from drug programs that promote harm minimisation – was dismissed as “a disgrace” and “frightening” by some anti-drug campaigners.
Gordon Moyes, the “Christian voice in politics” is also quoted on rumours in Drug Free Australia’s recent attack upon Lancet authors, of which Reece is a co-author. This involves quoting Moyes, who is quoting drug addicts he happened to speak to. Moyes also praised naltrexone despite the concerns of our medical community about it remaining unregulated. Regrettably, regulators have not prevented its use by the same people year in, year out.
When the Medical Journal of Australia exposed the fact these same prescribers were not reporting adverse reactions, despite TGA requirements under the Special Access Scheme, Drug Free Australia published a rebuttal. It made direct reference to Dr. Stuart Reece himself. Offensively, it reported that Reece “studies” death rates post naltrexone treatment. It was titled, Australia could be the biggest loser.
Dr. Reeceʼs motivation is arguably reflected in his obsession with teenage and childhood sex and sexual assault, murder, violence… all due to “the depraved advertising industry” which catalysed “the disease sex, drugs and rock-n-roll”. Advertising womenʼs nudity, outside of “a strictly medical context” is “incredibly powerful pornography”, he has observed.
Today, a decade plus since this evidence-free pursuit began, Reece is arguably a pin up boy for religious fundamentalism. Five or more years ago he promised Parliament that his results were “statistically powerful” and “revolutionary”. Of course, there are no results. Itʼs the same certainty that only faith can sustain. If prayer cures homosexuality, addiction is a certainty. His latest work “proves” naltrexone is safer than opioid therapy.
As reported on ABCʼs 7:30 Report, in 2006 multiple disciplinary teams have steadily found naltrexone has a fatality rate over four times that of opioid therapy. Dr. Reece, and others who seek funding and likely lucrative contracts seem to have a formula no others can find. More recent work with implants by his colleague, gynecologist George O’Neil, show ambiguous results, despite claims of success.
Regrettably this work is tainted with poor practice and again, Christian healing. Their biggest problem is the fraud published in the MJA surrounding suppression of negative outcomes – some almost fatal. Failure and coercion to boost sample numbers seems to be the norm. W.A.’s Freshstart clinic observes on its website chaplaincy page:
Our Christian Beliefs
The Nature and Character of God: we believe in one God, who has existed forever as Father, Son and Holy Spirit in a community of pure and eternal love.
The Fresh Start Statement of Belief embodies the second of the core commitments of the organisation:
The Creation of Humanity: men and women were created in God’s likeness with God-given dignity and worth in order to know, love and serve him forever.
Sin and Evil: sin came into existence through human rebellion against the good purposes of God. Sin is self-centred opposition to the love of God that separates humans from God and leads to death and eternal lostness.
Etc, etc….
There is no problem with having a strong faith. Yet there’s a difference between faith based welfare and faith based practices. When the supernatural impinges on your objective reasoning in managing the lives of others, no amount of friendly lobbyists can assuage this conflict of interest.
Today, Drug Free Australia bill Reece as “an expert in naltrexone” and in fatalities. Is this a joke? I honestly don’t know. What’s certain however is that his role in the recent DFA misleading outing to attack Vancouver’s Insite and the research backing it is not based upon any skill in harm reduction.
Drug Free Australia have many secrets. This one is quite shameful.
Comments posted online from a relative and a friend of Reeceʼs patients.
Just Jules says: June 5, 2010 at 6:01 am Ahhh there is none so blind as those who can not see .. Dr Reece in my eyes is a discusting (sic) human being .. I am the mother of a child he treated .. He also treated my daughter in law and the mother of my first grand child .. If you want to see what his methods leave you with, go see my daughter in law who for the last 11 years has been in a home for the severely brain damaged .. In is own words to me ” they are just reoffending drug addicts”. He is a wolf in sheeps clothing and should of been stopped before he started.
Vicki PS says: July 5, 2010 at 12:02 pm I came across this site looking for help for a friend of my daughterʼs. This young woman has been increasingly unhappy with her treatment under Dr Reece. He is treating her addiction with Suboxone, a subutex/naltrexone combination drug. Her big concern is that this unethical, immoral disgrace to the profession reduces her dosage if she has not been to church! This girl is now in early pregnancy and is scared that she could miscarry if this idiot messes around with her medication to suit his pathological world view. I find it frankly incredible that Dr Reece is still permitted to practice.
References:
MORTALITY RELATED TO NALTREXONE IN THE TREATMENT OF OPIOID DEPENDENCE: A COMPARATIVE ANALYSIS – NDARC (HTML) (Download PDF)
Unplanned Admissions to two Sydney Public Hospitals after Naltrexone Implants – MJA. (HTML) (PDF)
IMPACT OF ILLICIT DRUG USE ON FAMILIES: HOUSE OF REPRESENTATIVES – Tuesday, 3 April 2007 (Download PDF)
Australia’s National Drug Strategy consists of the three pillars of Harm Minimisation
To hear major parties speak of Australia’s national drug strategy one may be forgiven for assuming it is a competition of muscle. To be sure, we’ve come a long way since the great stupor of the Howard years, as then federal Health Minister, Tony Abbott taunted Opposition leader, Kim Beasley for being “soft on drugs”. Translation? Taking the evidence based advice of global drug strategists.
Terrified of losing votes, Beasley all too readily took the bait. In this way successive debates and policy changes had a ratcheting effect on absurd non evidence based and wasteful attempts to be seen to be “tough” on drugs. Manfully tearing up cannabis plants and thrashing them against rocky outcrops or cursing at bags of cocaine aside, it follows quite logically that “tough on drugs” is nothing less than tough on people.
Should Abbott become PM we will quickly find that there is more to Aussie politics than just carbon taxes, boat arrivals and the odd NBN slur. It wasn’t just Howard’s homophobia, weapons of mass destruction lies and black and white 1950’s relativism we’d woken up from. Howard’s skill as a politician is rivalled very well by his inability to understand the 21st century. Indeed, perhaps the last third of the one before.
I’m not suggesting drug policy should become a national focus to the exclusion of any other policy. It never will. Yet, the list of human rights abuses ushered in by stealth and without reason under Howard is a long one. It was Tony Abbott himself who funded the extreme right evangelical lobbyists, Drug Free Australia with the explicit aim of destroying Neal Blewett’s 20 year old successful policy of Harm Minimisation. Howard’s sabotage of our role as world leaders in Harm Reduction is legendary.
Even in 1997 going against the advice of then health minister Michael Wooldridge, and taking that of (later) DFA board member, evangelist and disgraced Salvation Army Major, Brian Watters (initial Chair of the ANCD) to dump the heroin on prescription trial. From The Politics Of Heroin – ABC 4 Corners:
KATE CARNELL: The approach that we put, or I put, to that meeting, was that this was a small trial, only 20 people or so in the first instance. That the trial would be a medical trial with appropriate science backup.
ANDREW FOWLER: The vote came as a huge surprise. The Federal Health Minister, four States and the ACT voted for the trials to go ahead.
A 6-3 result. The decision marked a radical shift in policy.
KATE CARNELL: This is not just a heroin trial. It’s an integrated, national approach that brings in the majority of States in this country. I think it shows a huge amount of maturity and it really is a mammoth step forward.
ANDREW FOWLER: The Federal Health Minister, Michael Wooldridge, telephoned the Prime Minister to tell him the news. But a few minutes later, as he made his way back into the meeting, observers say he looked shaken.
Nothing to this day has beaten Bronwyn Bishop’s 2007 Parliamentary Committee Inquiry. A despicable abuse of our parliament and the role of standing committees, the final report was rejected by every D&A body in Australia. All except our installed enemies of humane policy, lobbyists Drug Free Australia. As Chair and at John Howard’s urging she intoned to field experts that, “the PM says he doesn’t want that” (Harm Minimisation), sounding much like an Inquisitor instructed to reject reference to heliocentrism. That this was her governments policy was entirely lost on her. It was a predetermined farce to attack progressive successes, and demonstrably so.
Her attacks upon Alex Wodak‘s internationally respected skill and evidence in favour of biblical stories from fundamentalist zealot Dr. Stuart Reece, left jaws agape. A bastard baptising, bible wielding, Jesus summoning fruit cake who’d knocked off 25 of his patients in 20 months with reckless naltrexone treatment. The investigation into which he described as “a conspiracy”. “They’re only drug addicts anyway”, he informed a grieving parent who later wrote to me.
In lengthy evidence to a current parliamentary committee inquiry into illicit drugs, being run by Bronwyn Bishop, Reece suggested one of the biggest problems at the moment was a disease called “drugs, s-x and rock and roll.” As part of his evidence, Stuart Reece cited Sodom and Gomorrah, the Biblical cities destroyed by God for their immorality.
Reece’s testimony then suggested Australia’s civilisation was under threat of being destroyed by the scourge of injecting rooms, give-away syringes, and methadone. These of course are the well-established strategies of “harm minimisation”, the approach that underpins the way Australia deals with the dangers of illicit drug use. In contrast to his attacks on harm minimisation, Stuart Reece spoke reverentially of the work of Dr George O’Neil, and the immense value of the still unproven naltrexone implant.
Asked during an interview whether he currently prescribed naltrexone implants to heroin addicts, Dr Reece answered cryptically, “Yes and No”.
Suffice it to say, Reece as a member of Drug Free Australia still marches front and centre with the most dangerous and most irrational opponents to Harm Minimisation. Our National Drug Strategy. What they call “the noramlisation of illicit drug taking”.
However, the Public Health Association report below on the proposed Needle, Syringe Program (NSP) trial at the Alexander Maconoche Centre is clear:
The Australian government web page on the National Drug Strategy (NDS) identifies that
“the National Drug Strategy, a cooperative venture between Australian, state and territory governments and the non-government sector, is aimed at improving health, social and economic outcomes for Australians by preventing the uptake of harmful drug use and reducing the harmful effects of licit and illicit drugs in our society”. (Australian Government Department of Health and Ageing-DoHA, 2011)
The NDS is based on three inter-related strategic approaches to dealing with drugs in our community – the NDS refers to them as the “three pillars” of the overall approach of harm minimisation.
Harm minimisation, therefore, is our agreed national approach to drug policy which encompasses the three pillars of:
Demand Reduction
Demand reduction to prevent the uptake and/or delay the onset of use of alcohol, tobacco and other drugs; reduce the misuse of alcohol and the use of tobacco and other drugs in the community; and support people to recover from dependence and reintegrate with the community. To achieve this requires effort to:
prevent uptake and delay onset of drug use
reduce use of drugs in the community
support people to recover from dependence and reconnect with the community
support efforts to promote social inclusion and resilient individuals, families and
communities
Supply Reduction
Supply reduction to prevent, stop, disrupt or otherwise reduce the production and supply of illegal drugs; and control, manage and/or regulate the availability of legal drugs. To achieve this requires effort to:
reduce the supply of illegal drugs (both current and emerging)
control and manage the supply of alcohol, tobacco and other legal drugs
Harm Reduction
Harm reduction to reduce the adverse health, social and economic consequences of the use of alcohol, tobacco and other drugs. To achieve this requires effort to:
reduce harms to community safety and amenity
reduce harms to families
reduce harms to individuals
Our NDS does not simply limit its scope to the broad community but states categorically:
“The approaches in the three pillars will be applied with sensitivity to age and stage of life, disadvantaged populations, and settings of use and intervention”. (DoHA 2011)
Over the years we’ve had the rants of Alan Jones and John Laws. The rubbish of Piers Akermann and Andrew Bolt. The fear mongering of the anti-science mob. Still many fail to appreciate not just good policy but the responsibility under human rights which (as I’ll get to in time) is exactly what Alexander Maconochie is about. Right down to using the name of the great penal reformer himself.
This Lateline segment from October 2009 gives excellent insight. On October 2nd 2009 they reported, “The Australian drugs conference in Melbourne has today called for a trial of needle and syringe programs in Australian prisons. One in three Australian inmates has hepatitis C, and it is thought that a needle and syringe program could reduce the incidence of blood-borne viruses in jail.”
Resistance born of political will, not evidence, continues today. It will be a great shame if ignorance prevails.
Lateline
Public Health Association Report on NSP Trial at the Alexander Maconochie Centre
Needle Syringe Programs in prisons have proven successful across the globe, including in Iran. Gains are directly transferred to individuals, family members, community members, custodial officers, law enforcement officers and health professionals.
Australia once led the world in Harm Reduction initiatives, a number of which pertain to safe injecting of illicit drugs.
Because of the illegality, potential for tragedy and high risk associated with IV drug use it is very easy to be led astray from the evidence base supporting harm reduction initiatives. Primary amongst these is the funding of over 1,000 Needle, Syringe Programs (NSPs) across Australia. Although introduced against considerable opposition, community acceptance is now very high. More to the point, similar misinformation and conservative opposition was raised against another harm reduction initiative when introduced. Condom use amongst men having sex with men (MSM).
Harm Reduction measures were introduced by then federal health minister, Neal Blewett in 1985, ushering in unprecedented acceptance, understanding and management of high risk behaviour leading to the spread of HIV in Australia.
Led by the Minister for Health under the Hawke government, Neal Blewett, Australia undertook several unprecedented and pragmatic steps: it introduced a needle exchange program for intravenous drug users, encouraged open discussion of safe sex, and created the famous Grim Reaper advertising campaign.
There was fierce opposition from the religious right, but 25 years after the initial AIDS outbreak, Australia’s decision to accept human nature in policy making has saved thousands of lives – especially when compared to the USA where ‘morality’ has outweighed practicality in dealing with the illness.
Harm Reduction (HR) is one of the three major prongs of Australia’s illicit drug policy. The policy is called Harm Minimisation. Not “tough on drugs”, not “zero tolerance”. Harm Minimisation includes Supply Reduction, Demand Reduction and Harm Reduction. Over the years the gay lobby and LGBTQ community has forged itself a formidable legal and social identity. I pity the conservative zealot who would insult their ontology. Not so for IV drug users. This is due to many reasons, the more obvious being the transient nature of drug use (experimentation), the social, professional and personal cost of outing oneself as a chronic addict, the complete lack of intention to politically mobilise and the volume of comorbid mental health problems.
To be rather crude whilst it is demonstrably bigoted to discriminate against Australia’s disabled population they are not a force of reckoning. Our communities remain poorly suited to accommodate disabilities. Stigma persists leading to discrimination and inequality.
Similarly whilst we clinically accept the disease model of addiction, many community members still remain blinded to this very real health problem in favour of pop culture “bad guy” stereotypes. This is sheer manna for those with political interests to be seen to be “tough on drugs” or who seek to exploit individuals with a range of disabilities, including drug dependence.
Most Aussie addicts are alcoholics and cigarette smokers. The bulk of public health money dealing with drug induced harm is spent here. Illicit drug addiction consumes under 5% of the total expense. Writing in, Redefining Addiction in MJA Insight Paul Haber noted:
The American Society of Addiction Medicine (ASAM) grappled with this problem for 5 years before releasing its new definition of addiction, which has stimulated interest from around the world with commentaries in The Lancet, Time and elsewhere. ASAM proposes that addiction is a primary, chronic disease of brain reward, motivation, memory and related circuitry. It is a chronic relapsing and remitting disorder that manifests in continuing use of substances or alcohol despite accumulating harm to the individual and to others. [….]
This addiction disease concept facilitates a medical approach to management, including the need for quality evidence to support clinical interventions and it encourages engagement of medical professionals in this field. Acceptance of the disease model can also reduce the stigma of the disorders. Specific neurobiological abnormalities have been identified such as certain dopamine receptors in the reward system and these are targets for therapeutic intervention.
The funding pittance that is dealt to illicit drug harm reduction in part reflects the dwarfing of this demographic alongside drinkers, smokers and gamblers. The rest is explained in that the lions share is consumed by futile supply reduction efforts in the endless cycle of importation, distribution, dealing and administration. Demand reduction – fighting the demand for drugs through education, rehabilitation and disincentives also receives more money than harm reduction. It remains far, far too easy to raise a voice of ignorance and accuse HR initiatives of “allowing” or “encouraging” drug use.
The ABC news items below discuss the need for needle exchange programs in Australian prisons and the potential for a trial beginning in Canberra’s Alaxander Maconochie prison. It’s probable an HIV epidemic beginning in injecting drug users, and placing the wider Australian community at risk, would begin in Australian prisons. Questions are also raised as to the “shameful” state of Australia’s Harm Reduction initiatives that have fallen behind what is considered effective evidence based practice for prison population health. This is further evidenced by successful programs in other countries around the world. Needle Syringe Programs are strongly supported by a large global evidence base. Significantly, one public health success story is Australia.
Indeed return on investment research in 2009 [PDF] show that “investments in needle and syringe programs were yielding a twenty seven fold return in health, productivity and other gains.” Gino Vumbaca, Executive Director of the Australian National Council on Drugs wrote at the time:
What is striking is the level of public support for the program. The largest regular survey on drug use issues we have, the National Household Survey on Drugs, now records public opposition to the program at less than 20%. The Hawke, Keating, Howard and now Rudd Governments, as well as a myriad of state and territory governments of varying hues over the past 20 years have all lent their support to the program. For some this was in the face of strident opposition. A truly admirable achievement based on evidence, common sense and humanitarian grounds
The World Health Organization commissioned a review of evidence of the effectiveness of Needle and Syringe Programs to reduce HIV which concluded:
There is compelling evidence that increasing the availability and utilisation of sterile injecting equipment for both out-of-treatment and in-treatment injecting drug users contributes substantially to reductions in the rate of HIV transmission. Research from around the world clearly indicates that NSPs make a significant contribution to preventing the spread of HIV/AIDS and hepatitis C.
Between 2000 and 2009, the Australian Government invested $243 million in Needle and Syringe Programs. This resulted in the prevention of an estimated 32,050 new HIV infections and 96,667 cases of hepatitis C. $1.28 billion dollars were saved in direct healthcare costs. [….] The report states: “If NSPs were to decrease in size and number, then relatively large increases in both HIV and hepatitis C could be expected with associated losses of health and life and reduced returns on investment. Significant public health benefits can be attained with further expansion of sterile injecting equipment distribution.”
Countries, like Australia, that have implemented NSPs have averted HIV epidemics among injecting drug users and, therefore, the community at large. Those countries that have not implemented these measures have often experienced uncontrolled HIV epidemics. There is strong evidence to suggest that when HIV becomes endemic among the injecting drug user community it can then spread to their sexual partners and children, resulting in high mortality rates and large social and economic costs to the entire community.
Conservative ideologues and those with vested interests in punitive measures, have attempted to discredit NSP efficacy. Nations without proper NSPs, such as Sweden are deemed in breach of the UN International Right to Health. See page 3, item D. Religious fundamentalists & other totalitarian belief systems frequently reference Sweden’s “war on people” mentality, obfuscating the human rights abuse. As revealed by WIKILEAKS, the USA work actively to sabotage Harm Reduction initiatives as part of their War On Drugs policy, citing Stockholm as a reliable ally. An excellent discussion of this matter is to be found at Neurobonkers. The Global Commission on Drug Policy has demonstrated the failure of the Drug War. [CNN News]
With respect to needle exchange, rather than advance challenges to NSP efficacy with new research the tactic of a small minority is to attack existing methodology in an out of context, subjective fashion creating the illusion of an argument. An analogue today might be “pertussis diagnoses have increased, therefore the vaccine is ineffective” – a claim advanced by comparison of unrelated data sets.
In May 2010 Norah Palmateer et al. produced a meta-analysis using what they called “Critical appraisal criteria” to challenge the methodology of NSP research. However, even whilst selecting particular modes of distribution and leaving out others, a conclusion that “New studies are required to identify the intervention coverage necessary to achieve sustained changes in blood-borne virus transmission”, was delivered. This is scarcely revolutionary, yet is falsely cited as discrediting NSP efficacy by fundamentalist conservative groups. In truth Palmateer et al actually argue for a shift in analytical focus to biological rather than behavioural data. More so, they write:
The findings of this review should not be used as a justification to close NSPs or hinder their introduction, given that the evidence remains strong regarding self-reported IRB and given that there is no evidence of negative consequences from the reviews examined here. [….] We recommend a step change in evaluations of harm reduction interventions so that future evaluations: (i) focus on biological outcomes rather than behavioural outcomes and are powered to detect changes in HCV incidence; (ii) consider complete packages of harm reduction interventions rather than single interventions; (iii) are randomized where possible (preferably at the community level); and (iv) compare additional interventions or increased coverage/intensity of interventions with current availability.
“The findings of this review should not be used as a justification to close NSPs or hinder their introduction”. Yet this is exactly what the enemies of reason have done, misquoting Palmateer at every turn. The “AVN” of Blood Borne Virus control is a group of far right evangelical lobbyists known as Drug Free Australia. Their “Meryl Dorey”, as it were is their “secretary”, young earth creationist and climate change denialist, Gary Christian. The similarities between Dorey and Christian are striking. No medical or health qualifications, citing of global conspiracies, “social experiments” – not evidence based public health, saving Australians, provision of “truth”, attacking certain research identities, cherry picking of data and outright lies.
When a 27 fold return on investment for NSPs was claculated after years of research, Mr. Christian promptly dismissed this claiming NSPs actually serve to promote drug use and spread viruses. WHO data would prove this if properly adjusted he cried, mimicking Dorey’s claims to “properly read research”. Thus he was able to immediately dismiss what is absolute proof opposition to NSPs is baseless. Indeed, Christian went further.
Harm Reduction is the “normalisation of illicit drug use” not just correlating to, but causing a rise in drug use. Hands up if knowing about NSPs motivates you to experiment with IV drugs. This new take on “condoms cause AIDS” is demonstrably flawed. Just as abstinence, not condoms will prevent STD’s, Christian claims “free HIV testing” not NSPs or harm reduction will control HIV, citing discredited non peer reviewed sources.
Thus arguments raised against the value of exchange program efficacy in cutting blood borne virus spread are emotive, supposedly backed by misrepresented, spurious and/or biased “research” and driven by discredited, conservative fringe lobby groups.
Unsurprisingly the opposition to NSPs in Aussie prisons is based on misinformation and a lack of evidence.