Whilst we can blame the impact of the global anti-vaccination movement, an increase in vaccine hesitancy that arose and has persisted during and since the COVID-19 pandemic, and even some RFK Jr. flotsam misleading the gullible, when it comes to measles, Australia and Australians must be especially vigilant in managing the risk of infection overseas.
I’m not a doctor nor hold any position allowing me to claim I can advise you, beyond what I read, on any infectious disease. Indeed I would recommend speaking first with a qualified doctor about the topic. Measles is highly contagious and spread via respiratory droplets (aerosols). Non-specific symptoms such as fever, rash, nasal discharge and cough are common. Nonetheless measles has a reasonably high rate of complication leading to hospitalisation or death.
The role of measles infection in causing immune amnesia | 2 | is remarkably disconcerting. I’d urge any reader to invest even modest time to understand this phenomena, and ensure oneself and loved ones are immunised against this virus. Remember, there is no cure. Quaint stories from anti-vaxxers of them all having it as a child and growing up with no ill effects are possible only because they refer to pre-vaccine years and choose to forget the friends who never returned to school, became blind or sustained brain damage.
Today (31st March 2026) saw the Australian Centre for Disease Control (ACDC) publish a firm reminder that if you’re travelling OS, adding a measles jab to your pre-travel preparations is more than wise. Even if you’re sure you have been vaccinated in the past, if you can’t confirm this with records, consider yourself un- or under- vaccinated. Adolescents or adults born during or after 1966 are recommended to receive two measles containing vaccines at least 4 weeks apart [Source]. It’s also quite safe and more than sensible to top up your MMR, particularly if you’re an adult, and decades have elapsed since your initial MMR. First let’s consider this sub-heading from ACDC News.
A new report confirms that almost all cases of measles in Australia are either acquired overseas or related to an overseas acquired case – especially around school holidays. Don’t bring measles home from holidays – add vaccination to your travel plan.
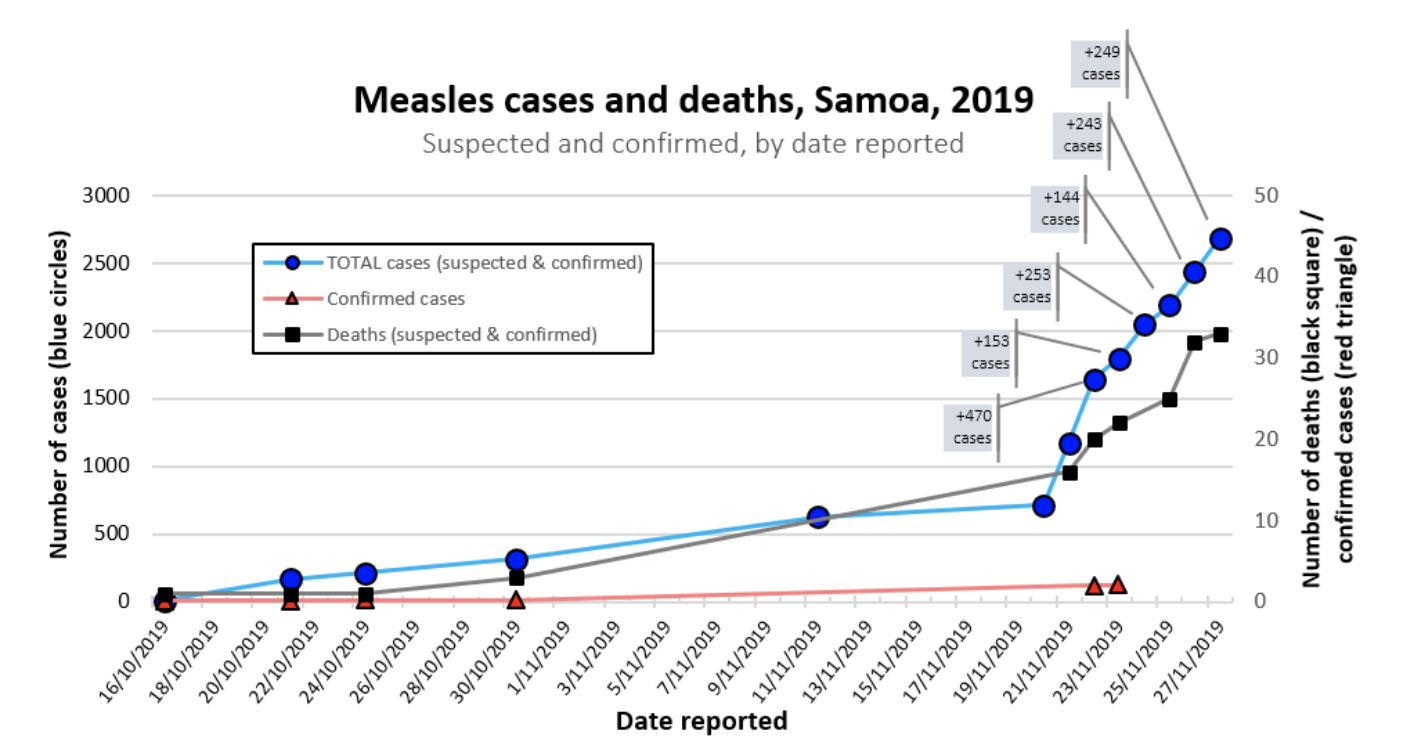
In fact the report | PDF | scrutinising the decade to 2024, reveals the years of highest infection were 2014 (339) and 2019 (284). There were 1,095 cases of infection reported during that decade. Almost all cases had either been acquired overseas or from someone who had brought measles back to Australia from overseas, states the ACDC news piece.
Further breakdown of figures tell us that when it comes to vaccination status, that 47% were unvaccinated, 30% had an unknown vaccination status, whilst 14% were under-vaccinated (being one dose). This final figure reinforces the importance of completing a vaccine schedule as well as confirming the impact of even insufficient antigen stimulus delivered via vaccine. The smallest number of infections were seen in subjects who had received only one of the two required measles shots. Measles infection was most common in those who had travelled OS – particularly to countries where measles was common. 57% of total notifications were in people aged 20 to 49 years.
2025 and 2026 data confirm a striking increase in measles infection. The total for 2025 was 181 cases. Currently we’re 25% of the way through 2026 with data showing 85 cases. This puts us on track for a 2026 total of 340 measles cases. The report also noted the drop in childhood measles vaccination from 94% in 2020 to 91% in 2024. Rather than look at this as a drop of only 3%, we must remain aware that measles herd immunity is impacted negatively when immunisation drops below 95%. So in reality, the reduction in immunisation has been steadily placing us all at greater risk since 2020.
Indeed certain groups are at higher risk of harm from insufficient herd immunity, including:
- The immunocompromised
- Those unable to be vaccinated for short or long term
- Children too young to be vaccinated
- The pregnant
Clearly, it’s important to plan some weeks ahead of travel as the two MMR (or measles) shots need to be given at least four weeks apart. Even if urgency applies, a gap of two weeks is insufficient to promote an adequate immune response. If an infant under 12 months needs to be considered for OS travel and/or an MMR course please see a paediatrician or your General Practitioner. On that topic, this NCIRS FAQ page is an excellent resource. It includes:
Infants travelling overseas can receive an early dose of measles-containing vaccine from 6 months of age, following an individual risk assessment, in addition to the routine doses given from 12 months of age.
Global outbreaks have been on the rise for some time. Australia has been keeping pace as best it can. Each state and of course the country as a whole is seeking to promote vaccine uptake and keep a close eye on the impact of outbreaks. There is only one solution and that is an increase in immunisation across the nation.
References below are from different states, news items and excellent US herd immunity/outbreak simulators.
- Measles cases almost triple in Australia as global outbreaks continue – ABC, 22/12/2025
- Increased risk of measles in Victoria – Vic Dept Health: 22/02/2026
- Free Measles Vaccine for Victorians – 4/03/2026
- Measles Alert in NSW
- Measles Alert for Brisbane Airport – 25/03/2026
- QLD: 10 cases acquired OS and 5 cases acquired locally – 30 March 2026
- Measles Alert – W.A. Government: 16/03/2026
- Measles Epidemiology in Australia – Full Report
- CDC Measles Outbreak Simulator
- FRED US Measles Simulator
- Herd Immunity Simulation: 2015 – Guardian