Skepticon Australia 2025 is to be held at the Forum Theatre in Melbourne over the weekend of 4-5 October. There’s also a Friday night meet and greet on the evening of the 3rd. Tickets are now available.
The speakers list is steadily growing. The Skepticon page tells us:
This is the twelfth Australian Skeptics convention to be held in Melbourne.
Renew old friendships, make new ones, and hear from the best speakers at Skepticon XL.
The 2025 convention will be held on the weekend of October 4-5 at the Forum Theatre, University of Melbourne, a great venue a few steps from the newly constructed Parkville Underground train station.
You can expect another line up of high quality speakers giving skeptical perspectives on medicine, science, education, belief and consumer issues. Guaranteed to be informative, incisive, challenging, and lots of fun.
Stay tuned for information about the Friday night meet and greet and the Saturday night dinner.
It will be a festival exploring science, reason, critical thinking and skeptical conviviality.
I can recommend the event, and advise keeping an eye on the Skepticon site as finer details about speakers, topics and the Saturday night dinner take shape.
It seems longer, but it has been only two and a half months, since we dropped in on Monica Smit and her self-appointed government-in-waiting, absurdly named Reignite Democracy Australia (RDA).
The occasion was their attendance during COVID-19 lockdown at a meal held at Moda Kitchen and Bar in Seddon, in breach of the Victorian Public Health and Wellbeing Act 2008. It was all a bit of a chuckle, given that the group effectively outed themselves and the restaurant by boasting about it on social media. The amusement was short lived for Moda however. On 6 August they announced their imminent closure on Instagram and Facebook. Their last meal was 14 August, just 11 weeks after hosting RDA. A representative told Star Weekly that the closure was unrelated to that event.
The representative claimed that mask-wearing mandates and lockdowns had not effected the business, insisting, “To be honest, we’ve never been so busy”. Although the attitude of the establishment to public health regulations was echoed in the observation:
Running a business is hard work and with or without the unlawful restrictions we were ready for a change.
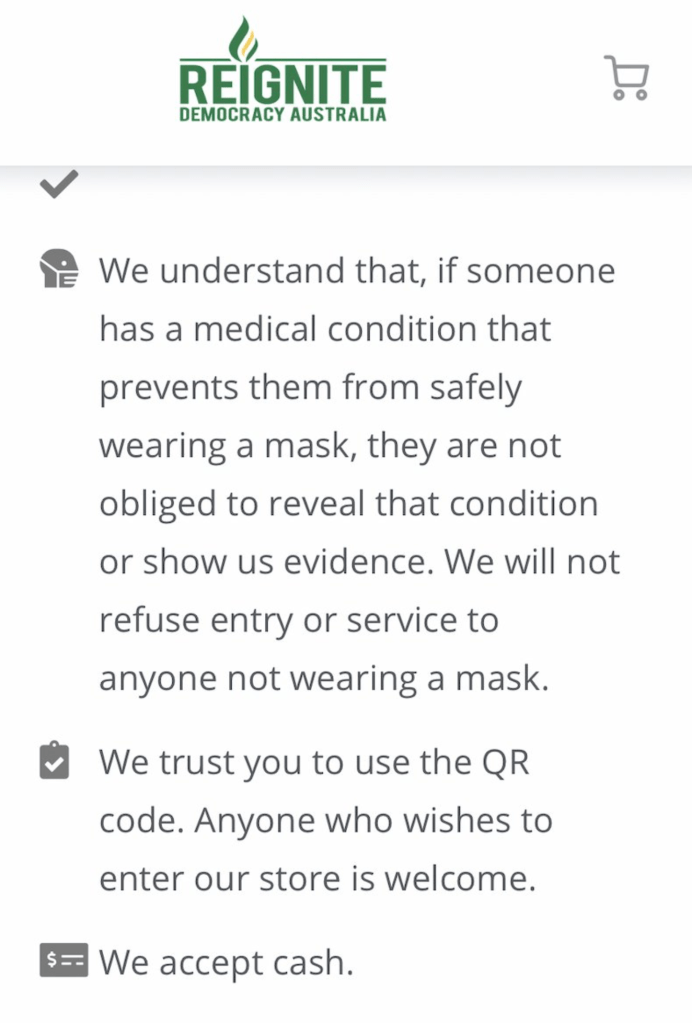
Speaking of unlawful, it should be noted that Moda Kitchen and Bar had made the RDA business listing. The listing provides details of businesses, prepared to exploit loopholes in public health regulations that keep us safe during the COVID-19 pandemic. Most specifically, this relates to mask-wearing and QR code check-in. There are exemptions to the requirement to wear a face mask. These include breathing difficulties, facial skins problems, intellectual disability, mental illness and having experienced trauma. The Privacy Act 1998, The Disability Discrimination Act 1992 and The Equal Opportunity Act ensure that no-one, should they not be wearing a mask, can be asked to provide evidence of such a disability unless their prior consent has been given.
It is thus quite easy for the dishonest to venture out without a mask. This is something we’ve seen as mask-less RDA disciples with phone cameras taunt police. The business listing idea is fluffed up through RDA concern that businesses might not be aware of the risks of discriminating. When it comes to QR code compliance, a business may simply trust patrons to do the right thing. Or perhaps trust them to do what Monica advises; choose to check in with pen and paper and be trusted to leave genuine details. If you happen to be a business that regard essential public health initiatives as “unlawful restrictions”, as Moda did, your RDA business listing is this.
RDA business listing – Moda Kitchen and Bar
ABC Radio Nth QLD
Monica Smit offers unregulated “advice” about public health and wellbeing mandates. On 12 August 2021, Monica was interviewed by Adam Stephens during the Drive programme on ABC North Queensland. The reason for this was RDA “You Can Say No” pamphlet-dropping in Cairns. Dave, a small business owner, was interviewed prior to Smit. He wasn’t impressed and wasn’t fooled.
The flyer tactic backfired, as the only change in his behaviour was to place a sign outside his shop, reinforcing that no mask or no QR code check-in, meant no entry. That Drive programme is archived and Dave and Adam begin their chat at the 45:00 min mark. Next comes Monica Smit, introduced by Adam as Monica Schmitt. Text messages, read out after a news break, were unanimously negative. If you’d prefer the highlights package, grab this mp3 here or listen below.
Cairns resident objects to RDA flyers, Monica Smit (4min), Adam reads text messages (9:40)
RDA recently made the Daily Telegraph’s top ten list of COVID misinformation spreaders in Australia. You may thus wonder why the ABC would give them air time. I would rush to add that the Daily Telegraph (DT) is not equivalent to the US based Centre for Countering Digital Hate. The latter spent significant time and resources, collating information on those they ultimately termed the disinformation dozen. Nonetheless, the central thesis remains intact. Despite clearly fallacious claims that place the community at risk, well-financed groups and individuals manipulate Facebook to their advantage. The DT reported that RDA subscribe to the belief no COVID-19 vaccine has been properly tested, and in fact weaken the immune system.
They also allow their name to back the conspiracy theorist standard that the vaccines are “manufactured by people who openly want population control”. Professor Mary-Louise McLaws specialises in infection prevention and control. She rightly observed those claims were “completely fallacious” and “wickedly inaccurate”. In a welcome development since the DT piece on 6 August, RDA had their page, and shortly after their backup page, unpublished from Facebook. That came on the heels of their aggressive campaign to boycott SPC, after the fruit packing giant mandated COVID-19 vaccination for employees. The boycott campaign resulted in product tampering and threats that presently continue.
Editorial standards?
Adam Stephens did give his reasons for interviewing Smit. He observed that it’s interesting that there are people that hold this view. That there are people in regional QLD who are active members of RDA, as evidenced by pamphlet distribution in Cairns. He continued;
Whether you wanted to hear from Monica or not there are people that are listening to her message, and sometimes it’s… I think worthwhile in actually learning about the motivations of some of these groups in our community, and some of the people that feel strongly enough to actually join groups like this and distribute their information.
I’m aware that listeners took the trouble to contact the ABC to voice concern. Before we examine Monica Smit’s claims, let’s consider the following. Smit was not introduced with sufficient context to advise listeners that they may be misled. It was not stressed that Monica Smit and RDA are not medical or pandemic specialists or that they are not advised by medical experts. It was not explained that their website provides no reputable or evidence-based information. Indeed, it was not stressed that the group has no relevant qualifications specific to the management of COVID-19, or any illness, at all. Finally, there was no public health representative on hand to address the claims made by Smit.
One might then ask, were ABC standards for editorial accuracy satisfactorily met? Granted, a context of sorts was laid down during Stephens’ chat with business owner Dave. Whether this was enough to reinforce that Smit and RDA act in dissonance to both government guidelines and evidence-based health policy, is not merely unclear, but unlikely. Monica Smit brings a firm, if utterly misguided, confidence to her stints behind any microphone. It came to the fore as she insisted that masks were not only useless and causing harm but there is, “so much science out there” to support this.
“Because it’s the truth”
When asked why she is informing people that they don’t have to follow mask mandates or QR code check-ins if they choose, Smit replied, “Well because it’s the truth”. With QR codes she advises to manually sign-in or shop somewhere else.
In effect this would mean finding a shop that has adopted Smit’s loophole advice. As we’ve come to expect from RDA on evading mask wearing, she mentions PTSD, anxiety, depression – the “huge list of exemptions”.
She blames, “the coercion and the scare tactics of the police and the government”, for forcing those with legitimate reasons for exemption, into wearing masks. At no time did Smit offer a legitimate reason as to why Australians without a health condition can refuse mask wearing. Unless of course, you are willing to feign one (I’m not suggesting she advised this). She followed on by claiming long term mask wearing is “really dangerous”.
That word brings to mind the long debunked claim that oxygen is restricted and CO2 intake rises to poisonous levels. Smit gushes that “People have, you know, passed out at work”. A fan of Tucker Carlsen, Smit is likely influenced by the research letter pushed by him about six weeks ago, and now retracted from JAMA Pediatrics. Smit goes one better, claiming there is, “[A] lot of science to say that they cause cognitive issues with teenage children as well, and they’re wearing them eight hours a day”.
Smit might get that notion from an isolated German survey, looking at “complaints from adolescents and children caused by wearing a mask”. This is not “a lot of science”, and comes with an editorial note stressing the absence of a causal link. There is also the genuine concern related to the importance of non verbal facial cues, to children who are learning. These are minimised by face masks. Particularly in the classroom. As fate would have it, or rather, as science would have it, this has been studied pre-pandemic and during the pandemic. CNN published a handy summary here. If you land on the conservative City Journal, you will find arguably emotive material to support Smit’s contention.
Adam Stephens questioned Smit on whether she really did have substantial supporting science, given the evidence-based source material that advises government policy. Smit was glad he asked because in March and April of last year the media, “were saying that a healthy person wearing a mask is an absolute waste of a mask”. She wondered “why the narrative has changed”. In fact that was because of a WHO-funded systematic review and meta-analysis, published in June of 2020 in The Lancet. More so this was clearly conveyed in “the narrative” presented by the media. Consider this non-ambiguous heading in The Guardian: Victorians may be now be told to wear face masks to halt COVID-19 – what’s changed? Then Smit confidently offered another disingenuous and factually wrong line.
The ‘Brett Sutton’ lie
Smit claimed:
I know that Brett Sutton, he’s the Victorian CHO (Chief Health Officer) here, he actually did a full study paper on how useless masks are to stop the spread of disease. So basically the narrative has just changed but the science has not changed and that is that masks are dangerous.
A “full study paper”? Sounds impressive. Also, I happen to agree with Monica here. The science has not changed. Nor has the old tactic of cherry picking and manipulating facts to support disinformation. What we find on checking Sutton’s authorship of research, is a 2001 literature review in Anaesthesia and Intensive Care, that he co-authored. At the time Sutton was based at North West Regional Hospital in Burnie, Tasmania. Both he and his co-author worked in the Department of Anaesthesia. The title of the literature review was Do Anaesthetists Need to Wear Surgical Masks in the Operating Theatre? A Literature Review with Evidence-Based Recommendations.
The review text could not be more clear. It was undertaken due to the absence of published data on the unmasking of the anaesthetist alone. In the modern operating theatre, exactly how this would impact post operative wound infection, if at all, needed elucidation. It was noted that surgical masks offer incomplete protection from bacteria and viruses. More so, plastic face shields provide better protection from infection for the anaesthetist. Three compelling studies, led the authors to conclude in part;
These studies provide sound scientifically-based evidence that, in the setting of a modern operating theatre with laminar flow/steriflow systems, surgical masks should no longer be considered mandatory for anaesthetists and non-scrub staff during most surgical procedures.
There is a reason for the extra detail on this review. This claim about Brett Sutton’s past authorship is not just misinformation, already tossed about like a Frisbee at a church picnic. This is hot-off-the-tongue disinformation. A nice fresh lie still in its packaging, delivered over the airwaves for the gullible to snatch up, unwrap and distribute. It has the added connotation that Victoria’s CHO is not only aware that masks are ineffective, but had produced “a full study paper” to this effect. Listeners may wrongly assume this is both recent, and in response to the COVID-19 pandemic. Smit studiously avoids admitting the paper is nineteen years old, and that it examines only anaesthetists and non-scrub staff, in operating theatres. Whilst cherry picking, she missed the one that suggested plastic face shields offer better protection.
In July 2020 Brett Sutton presented advice on wearing face masks, in areas experiencing stage three restrictions. At the same time the reasons for the mandating of mask wearing were being thoroughly discussed in mainstream media. It was impossible to miss. To suggest there was just a sudden change in “narrative” is wrong. Adam Stephen put it to Smit that her advice could place people at risk of COVID-19.
Deep breath
Without drawing breath, she responds;
Well I just totally disagree with that because, um, you know I think the government is putting people at risk of serious problems ah, with lockdowns and things like that so, it’s proven around the world that lockdowns don’t work. Australia has the worst lockdowns actually, I think, in the world. We’re being laughed at overseas because of how harsh our lockdowns are. Some, some, some countries have hundreds of thousands of cases daily and they’re still living about their lives, and we get one case and we close borders.
So ah, I would say the government is being a lot more dangerous than we are, and we’re actually empowering people to have critical thinking, which the government doesn’t want. They don’t… the government’s not giving people all the information. And that’s… and we get censored. I just got taken off Facebook. I had sixty six thousand followers and I get censored because my science is apparently not true, but I can back it up. But a lot of the science that’s said on mainstream media can’t be backed up but there’s no censorship for them so it’s really difficult.
It has not been “proven around the world” that lockdowns are ineffective. They remain one of the most effective non-pharmaceutical interventions. Healthy discussion continues about how this effects economies and communities. What is doubly strange about Smit’s approach here is that if masks are as useless as she claims, there is one clear alternative. The very lockdowns she also insists are useless. I doubt she is aware of this. Her approach is to attack all options, and encourage us to abandon them. She has no alternative to offer Victoria.
Stephens raises the question of people who accept the claims on the You Can Say No flyer, being fined. Smit comes back with a prompt that all the resources are on the website, and that;
If you get the flyer you really need to take that extra step to actually do the research because if, you know… know the law and you know your rights, then actually that fine is null and void and it’s actually um… it won’t mean anything.
Adam lets Monica know they’ll leave it there. Smit responds with an eager “No worries!”. Those familiar with Monica Smit might have noticed the big grin-tone in her final words. She had reason to feel smug, as Australians have every right to expect better from our national broadcaster. Smit usually only gets this much air time on Sky News. The reaction on Telegram, the favoured social media platform of COVID conspiracy theorists, was predictable. Discussion was kicked off thirty minutes later by RDA on their Telegram channel, with an announcement headed by a customised graphic.
Telegram
The first post I wrote on Monica Smit and RDA, opened with Monica Smit loves being the centre of attention. That entire topic requires a post on its own. Suffice it to say however, that certain personalities only take. They surround themselves with givers, and ruthlessly ban, delete and expunge those who challenge their bogus view of reality. The result is the unfettered pseudo-worship you see in the small sample above.
Note the suggestion from one, to “destroy those imbeciles”, in reference to Dave the shop keeper. It’s further worth noting RDA didn’t provide Adam Stephens’ interview with Dave, or the dissenting text messages. All that was known is that a shop owner was “appalled” by the flyer. Sophie, who unwittingly outed herself as a Cairns local, and likely a distributer of the flyers, decided that was enough for the destruction of “those imbeciles”.
Still no evidence
The bulk of RDA members on social media, continue to behave as if enjoying a sustained muck up day. This, however, gives an inaccurate view of the groups resources. Their recent advertising truck, growing range of merchandise, and increasingly slick video production suggests donations remain healthy. This has enabled the group to curate their campaign of alienation through misinformation. Their message is for those who prefer to be told what to think, rather than make their own conclusions. Yet this group is convinced they have discovered a unique truth that “sheeple” cannot see.
Although Smit talks of access to science that confirms the RDA position, there is none on their site. The well examined Danish study on mask wearing and transmission of SARS-CoV-2, can be accessed in favourable format. Rather than finding masks do not prevent transmission, the study failed to find, “at least a 50% protection against a SARS-CoV-2 infection given by mask wearing”, as it was designed to do. Fact Check also addressed this nine months ago. In targeting COVID-19 vaccine safety and efficacy, RDA direct readers to the tired example of the estimated study completion date, for the AstraZeneca vaccine. The actual study completion date was 5 March 2021.
Other material is presented in misleading context. Despite Smit’s claim of enabling critical thinking, visitors to the site are shown bias. There are no opportunities to compare contentious information in a critical fashion. The elephant in the room here is that all reputable evidence is against the position held by RDA. The use of “critical thinking” as a buzz term, has become almost commonplace in conspiracy theory circles. It is seemingly confused with contrariness. This is underscored by the fact that constant cries of suppressed freedom, and the exploitation of loopholes, is possible only because of our democratic rights and the legislation that protects them.
Conclusion
There’s little point rambling on much more dear reader. I’m certain the RDA site would be worthy of content analysis. A work similar to the excellent approach employed by Thomas Aechtner, in assessing the Australian Vaccination-risks Network, would be welcome.
Monica Smit is more than just dishonest. In taking advantage of a global pandemic to raise her profile and profits she has proven to be a malignant influencer. What has been demonstrated above, is that everything Monica Smit said during the interview with Adam Stephens, is demonstrably false. More to the point it has long been clear what she stands for.
The Australian Broadcasting Corporation needs to be out in front of such people.
The Lancet VOLUME 395, ISSUE 10242, P1973-1987, JUNE 27, 2020. Physical distancing, face masks, and eye protection to prevent person-to-person transmission of SARS-CoV-2 and COVID-19: a systematic review and meta-analysis.
Corona children studies “Co-Ki”: First results of a Germany-wide registry on mouth and nose covering (mask) in children – DOI: 10.21203/rs.3.rs-124394/v3
These days social media is seething with COVID related disinformation and misinformation. The last week however brought out the best of the worst in those intent on denying reality.
Without a doubt last weekend’s protests in Melbourne, Sydney and Brisbane left some as excited as a lonely school kid might get after their first school dance in long pants. That does not explain the nonsense that followed however. That comes down to the antivaxxer, COVID conspiracy theorist trait of seizing a splinter of fact and presenting it in a way to support a broader deceit. The week’s carry on was unique for a couple of reasons. Firstly only a meagre understanding of the subject matter was needed to grasp the reality. Also corrections and clarifications were available in almost real time.
NSW, COVID-19 and Vaccination
When it comes to grasping the situation with Australia’s COVID-19 vaccine rollout, things are simple: it’s well behind schedule. More to the point, the delay in shipping Pfizer vaccine has been a constant hum in our news cycle for months. This has been amplified by confusion around advice from the Australian Technical Advisory Group on Immunisation, which has seen changes in the recommended age groups for receipt of the AstraZeneca vaccine. In six weeks over June-July it changed from 50 years and above to 60 and above. ATAGI advice held firm when Scott Morrison suggested all Australians should consult their GP to consider getting it, then ultimately the age was lowered to 18 years and above in view of the raging Delta variant in Sydney.
There was the backlash over an 11 July COVID-19 advertisement which carried the text, “Covid-19 can affect anyone… Book your vaccination”. The woman featured in the ad’ was in the age group for which Pfizer vaccine was recommended. But supply wasn’t there. Last Friday NSW health minister Brad Hazard made a plea to other states for Pfizer vaccines. He was left disappointed. The point to this brief and tedious history lesson is that a meagre (that word again) attention span is enough to grasp that NSW is in serious need of COVID-19 vaccines. Until last Saturday that had to be Pfizer for under 60s. Additionally, the impact of COVID-19 vaccination in keeping people out of intensive care has been making news across the developed world. When NSW Health gave updates on COVID-19 hospitalisations during press conferences we quickly learnt the same success is evident here.
When Dr. Jeremy McAnulty misspoke
As we moved into last weekend a trend of sorts emerged as senior NSW Health physician Dr. Jeremy McAnulty presented his reports. On 22 July the seriousness of the Delta variant was underscored by the fact that of 118 in hospital, 28 were in ICU of whom 14 were ventilated. He reported that forty two were under 55 years of age and fifteen were under 35. On 24 July Dr. McAnulty reported that 139 people were in hospital. There were fifty five patients under 55 years of age and twenty eight who were under 35. He noted that of 37 patients in ICU, 17 required ventilation, 36 were unvaccinated and one patient had received one dose of AstraZeneca. It was a disturbing trend. Young Australians were being hit hard by the Delta variant and hospitalised in increasing numbers. In the intensive care unit nobody was fully vaccinated. One person was partially vaccinated.
This was what we had feared may come of a slow vaccine rollout. Without the protection of vaccination COVID-19 was making adults of all ages very ill indeed. On 25 July Dr. McAnulty had the awful task of announcing two COVID related deaths. A woman in her late thirties, and another in her seventys had died. One could see the softly spoken public health expert struggle over the words. He moved on to report 141 people were in hospital of whom 43 were in ICU, with 18 requiring ventilation. Continuing with the same data sets of previous press conferences he reported that sixty of those hospitalised are under 55 and twenty eight are under 35. He noted that of the 43 in intensive care one was in their teens, seven were in their 20s, three in their 30s, fourteen were in the 50s, twelve were in their 60s and six were in their 70s.
At this point viewers keeping track of the new disturbing trend knew what was coming. Dr. McAnulty will report on the vaccinated status of those in ICU. Which he did. However he misspoke and said, “All but one are vaccinated, one has received just one dose of vaccine”. It was however clear what was meant: all but one are unvaccinated. The ICU patient numbers had increased by six and there had been two deaths. Even for viewers not catching sequential daily updates (I know I wasn’t), it was clear this was a slip of the tongue. As outlined above, Australia has had a sluggish vaccine rollout. On that day only 15.8% of NSW residents were fully vaccinated. Being vaccinated was not the norm and certainly not for Aussies under 60. Yet it wasn’t until journalists were asking questions around half an hour later, that Dr. McAnulty was able to correct himself.
Here’s the two relevant clips run together.
By then no doubt anti-vaccine activists had edited out the few seconds they needed and gleefully hit social media. Taylor Winterstein who makes a living from bad influencing on Instagram posted this the next day.
You might have noticed how she struggles with numbers. Dr. McAnulty was referring to forty three people in intensive care when he misspoke. Not 141. This same mistake is repeated elsewhere in the antivax rabbit hole. As is the response that his correction was false. Either bogus or doctored or whatever they can grab to avoid the facts. No surprise there. Although there was one surprise. Del Bigtree was swift to tweet the video with a message to see the point where Jeremy McAnulty misspoke, proclaiming that, “all were vaccinated but one”. The reality was pointed out to him. An hour later his first tweet was deleted and he tweeted a correction acknowledging his mistake. “Since he made a correction I must too”, Bigtree offered.
This is reasonably significant in light of the fact Del Bigtree is responsible for a copious amount of disinformation and misinformation regarding both vaccines and COVID-19. He is firmly convinced COVID-19 vaccines are ineffective or worse. Credit where it’s due however. After all, Dr. Dan Wilson of Debunk the Funk is a former conspiracy theorist. The same credit can’t be given to Del’s Twitter followers. Most reacted like the proverbial End of World cult faced with a world that didn’t end. Their justifications covered all bases including denial and even transforming a correction into a retraction! Then there was that darn antivaxxer problem with the number 141.
This scene was played out in social media rabbit holes everywhere. Replies to Taylor Winterstein were equally stupid. Which is an achievement as Winterstein controls who can comment on her Instagram account. Fact checking followed. AAP published a review of the fake claim, an analysis and supporting evidence of COVID-19 vaccine effectiveness. CoronaCheck included it in their weekly update and AFP Fact Check published a comprehensive slap-down of numerous misleading sources. Nonetheless such calculated disinformation has the potential to harm Australian public health and even cost lives.
When it comes to pumping up disinformation like this, it’s always hard to pass by Meryl Dorey, founder of the Australian Vaccination-risks Network. She too had trouble with the 141 number and even re-employed Dr. McAnulty as a “politician”. Dorey also claims COVID hospitalisations and deaths globally and specifically Israel, the USA and Europe are fully vaccinated. That’s another version of the carefully crafted mistake seen courtesy of Alan Jones and Craig Kelly who failed to grasp a statistical reality, and were splendidly refuted by Paul Barry on Media Watch. It is an example of base rate bias or base rate fallacy. This video explains it very well.
A look back at this week isn’t complete without highlighting the COVID PCR kerfuffle. On 21 July the CDC alerted laboratories that they would retire-with-a-gold-watch the CDC 2019-Novel Coronavirus (2019-nCoV) Real-Time RT-PCR Diagnostic Panel. What most of us know as the COVID-19 PCR test. Polymerase Chain Reaction testing is highly accurate. The process identifies the genetic material of a specific virus. It does this in a way that is similar to providing a yes or no answer to the presence of X virus. It cannot give a this or that answer to the presence of X, Y or Z viruses.
Since the beginning of the COVID-19 pandemic the anti-science conspiracy lobby has pushed two absurd claims about the detection of COVID-19. The first is that it has never been isolated. False. The second is that the PCR test is so fantastically unreliable that it produces only false positives. False. What’s interesting about these claims is that if one believes the first, then the second is true no matter what test is used. This however didn’t stop COVID-19 deniers from trying to discredit the technology of the test as a means to more or less blame it for positive results they didn’t like hearing about.
Because of the closed nature of the PCR test, further resources and expense are needed to test for other viruses. This is ultimately why the CDC want to discontinue the PCR test at the end of 2021. This is done by removing its request for emergency use authorisation for the test from the FDA. The CDC still support the accuracy of the test. However by encouraging the use of multiplex tests single samples can be tested for a variety of viruses. For example influenza A, B and COVID-19.
Echoes from social media rabbit holes erupted. The claim was that the CDC withdrew support for the COVID-19 PCR test because it couldn’t distinguish between influenza and COVID-19. This then, and not closed international borders was why influenza cases had dropped dramatically. Links to the CDC alert were published with pride. Concepts of vindication were liberally mixed in with this sudden inability to read. G&B Lawyers’ conspiracy theorist Nathan Andrew Buckley made the news. Ali Haydar, Will Connolly (aka ‘Eggboy’) and Reignite Democracy Australia featured amongst many to spread falsehood. AAP published another great takedown and analysis. FactCheck have a particularly comprehensive SciCheck article on this. CoronaCheck included a debunking in the same piece that debunked the abuse of Jeremy McAnulty’s slip.
“There’s a little bit of misinformation going around”
I’m perhaps pressing my luck with the Fixated Persons Unit, but I’d like to share some vintage Meryl Dorey Gish Galloping about the CDC’s recent PCR alert. Delightfully she kicks off by warning that, “There’s a little bit of misinformation going around”. Well I hadn’t noticed, so I’ll be on the lookout. At one point Dorey fancies herself as a lab technician telling her audience, “Because we are using a cycle rate of forty to forty five, every single positive is a false positive”.
There’s an mp3 here for your collection, or you can use the player below.
Conclusion
The COVID conspiracy, anti-vaccination activist movement that thrives on social media continues to deceive. The last week saw two fresh examples of disinformation. One of which callously exploited an obvious error, corrected shortly thereafter, during a NSW Health press conference.
The COVID-19 vaccine is in fact an experimental medical procedure and because of this insurance companies have made void any claims relating to this “vaccine”.
The experimental trial in Australia runs until 2023 and thus it is only available due to an emergency use clause. Insurance companies are linking adverse reactions and deaths to this trial. As companies won’t pay out for injury and death due to experimental treatment it follows that such events following COVID-19 vaccination are not covered by hospital or life insurance.
Not a word of the above is true. Yet this notion is circulating on social media in the usual and predictable places. Despite it being demonstrably false and something one can refute for themselves in a few minutes, it is a notion with active supporters. Many others go further and contend that consent has not been given to be part of this experiment. Thus a breach of the Nuremberg Code is happening right before us.
Ethically relevant but not legally enforceable the Nuremberg Code remains semantically powerful. As such it is regrettably abused by anti-vaccine activists who have for years peddled the false claim that vaccines are not tested for safety and efficacy. It just so happens that global scrutiny of the development of COVID-19 vaccines also provided firm evidence of Phase III trials. This again refutes the anti-vaccine position and I touched on this last September. Yet as antivaccinationists are apt to do the facts have been twisted into falsehoods to support ongoing attacks on the COVID-19 vaccine rollout and to boost claims of further breaches of the Nuremberg Code.
Now, whilst this post isn’t focusing on Meryl Dorey and the Australian Vaccination-risks Network, it just so happens that she can assist us. On March 13th during an error-packed Under The Wire, Dorey presented a detailed performance outlining the absurdities that constitute the Nuremberg Code fallacy specific to COVID-19 immunisation. You may download the MP3 here, or listen below.
All of the points above popped up today in a thread on a COVID freedom fighter’s Facebook page. Elle Salzone is a feverishly active defender of anti-science beliefs. Elle moves from business to business, scheme to scheme and presently pushes ClearPHONE. Salzone and buddies sell the phone, claiming it provides the privacy necessary for today’s freedom fighters. How reliable a service it provides is uncertain. Elle fights with and also films police over her refusal to wear masks or remain in quarantine when necessary. But that’s okay if you decide to be a Sovereign Citizen. Elle is anti-COVID related responsibility. You can peruse her page for details on these pursuits.
Today one of her posts [Update: quietly deleted on 8 April] was screenshot by a tireless defender of reason, and thus came to my attention. It turned out to be an obvious forgery from this Allianz Product Disclosure Statement (PDS) and could be promptly demonstrated as such. The slideshow below is of the Allianz forgery and the two original parts of the document that were used in making it.
Salzone posts the forgery and states;
THIS IS EXTREMELY CONCERNING!!!!
Imagine getting the experimental shot thinking you’re protecting your health, then getting seriously injured and having no private health cover to help you and not being to sue because all vaccine manufacturers have been indemnified…
All to maybe protect you for a virus with a 99% Survival rate..
You literally can’t make this shit up..
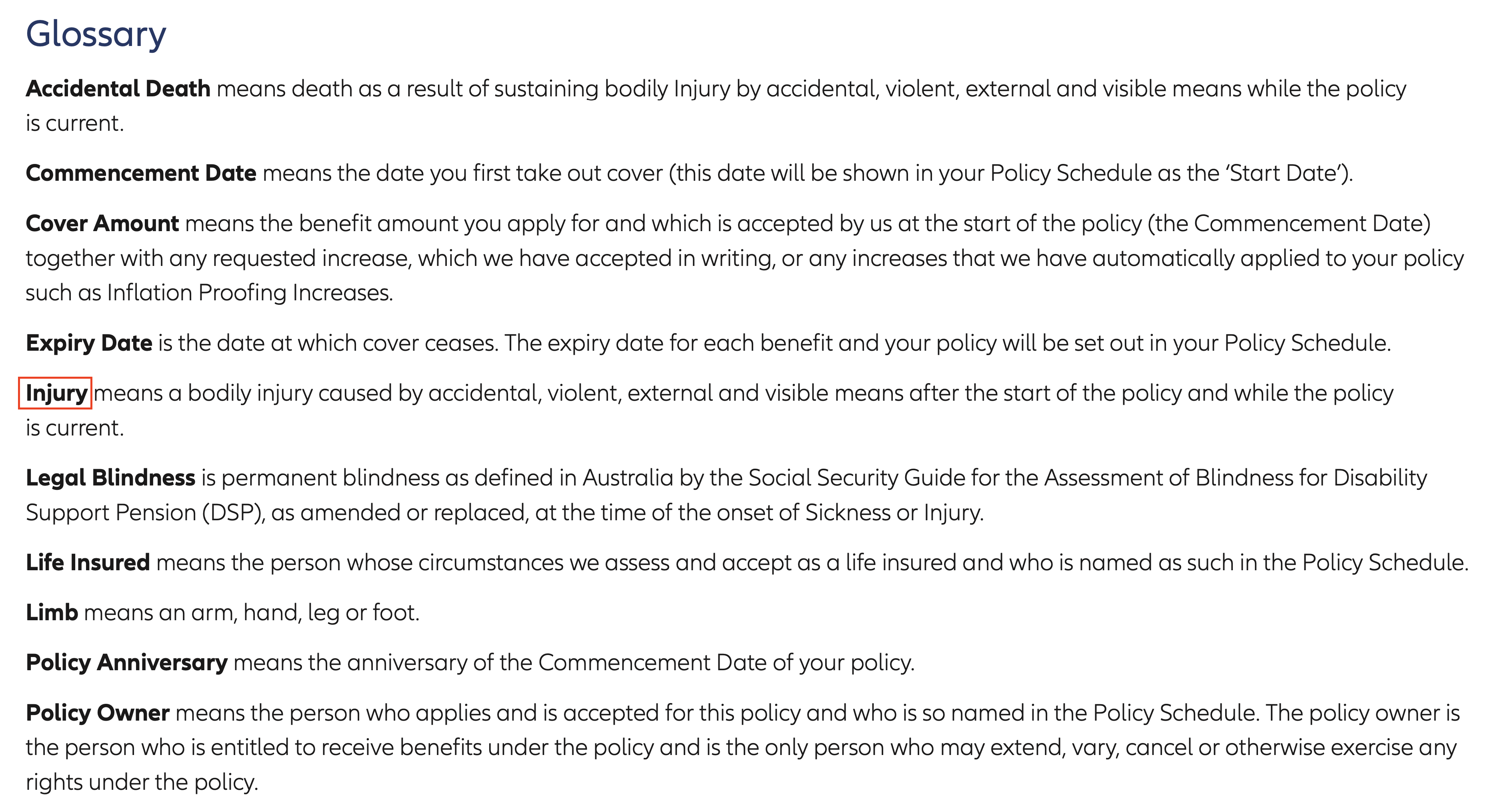
“You literally can’t make this shit up”. In fact you can and in this case someone literally did. A quick search yielded the document in question. Even before presenting the original, un-cropped and pre-defaced, pages the text itself was screaming forgery. Insurance companies do not tend to torment font in that fashion. Apart from the caps lock, no policy section is referenced. Then there is the sneer at “vaccine” and the impossible consent self-infliction. Ouch! Finally at risk of boring you there’s that nagging bit about posting this most important development in the glossary.
Suffice it to say the above points were mentioned and a discussion took place.
Verified by multiple sources eh? The original source was “easily found” (comment now deleted) but Elle couldn’t find it. So screenshots of the original source were provided along with a link.
This resulted in an admission that it was posted in the knowledge it was a fake. Apparently however the information it conveyed is not only true but would be confirmed by Allianz if I checked;
For the record this forgery consists of four different screenshots from the original document pasted in a sequence that creates a misleading ‘preamble’ aiming to justify the bogus claims made beneath in added red font. The added text further presents existing terms from the Allianz PDS to construct a fraudulent disclosure statement. A significant amount of time and forethought has gone into this. It is a calculated work of disinformation that has succeeded in misleading vulnerable recipients of its message. The preparation date of the current Allianz Life Plan PDS is 5 march 2021. The date in the forgery is 31 July 2020, suggesting it could have been in circulation for some time.
Perhaps the most important aspect to look at is the claim that COVID-19 vaccines are part of an experimental “medical procedure”. This is frequently peddled by anti-vaccine activists and was also pushed by Meryl Dorey in the audio above. It is linked to other claims that the vaccine is not actually a vaccine. One contention is that mRNA vaccines are DNA modifying agents. Another is that viral vector vaccines [CDC] are completely experimental and also alter DNA. Despite available data on the molecular action, development, safety and efficacy of Pfizer, Moderna and AstraZeneca vaccines, antivaccinationists ignore this in favour of a conspiracy theory.
Viral vector vaccines are well understood due to decades of research and do not alter DNA. mRNA vaccines are also well understood and are incapable of altering DNA. The claim that COVID-19 vaccination is an experiment is often presented with the contention that the experiment will go on until 2023. Like all persistent falsehoods this has an element of fact to it. The reality is that in Australia both Pfizer and AstraZeneca vaccines have provisional approval from the TGA. The approval is valid for two years and the AstraZeneca vaccine will require review in February 2023. On 16 February 2021 the TGA stated;
The Therapeutic Goods Administration (TGA) has granted provisional approval to AstraZeneca Pty Ltd for its COVID-19 vaccine, making it the second COVID-19 vaccine to receive regulatory approval in Australia.
COVID-19 Vaccine AstraZeneca is provisionally approved and included in the Australian Register of Therapeutic Goods (ARTG) for the active immunisation of individuals 18 years and older for the prevention of coronavirus disease 2019 (COVID-19) caused by SARS-CoV-2. […]
Provisional approval of this vaccine is valid for two years and means it can now be legally supplied in Australia. The approval is subject to certain strict conditions, such as the requirement for AstraZeneca to continue providing information to the TGA on longer term efficacy and safety from ongoing clinical trials and post-market assessment.
Reading the final paragraph above we can see also how the claim that data is still being collected for the experimental trial is peddled around with such confidence. Yet post-market assessment is a vital part to better understand all drugs and vaccines. There’s no trial, no experiment. It’s worth noting this fallacy is at times linked to another false claim. That of emergency use provision for the vaccine. This was a contention made by one Clive Palmer, deconstructed handsomely here by ABC corona check. Palmer has not alleged the COVID-19 vaccine rollout is an experimental medical procedure. Although he has pushed fear over the absence of one, three and five year safety data.
When it comes to hospital cover, insurance companies will not cover treatments for which no Medicare Benefits are payable. This includes cosmetic surgery, experimental treatments or experimental pharmaceuticals. Medicare will cover certain clinical research studies. For insurers if the device, trial or treatment is not recognised by Medicare or the Medical Services Advisory Committee it will be excluded from standard hospital cover. Still, there is insurance and indemnity available for clinical trials. This helps us understand why the term being used to misrepresent the COVID-19 vaccine is “experimental”.
Allianz also have a strong supportive position on the COVID-19 vaccine and like Bupa offer a comprehensive series of answers to possible questions. In a May 2020 article Allianz cover in depth the importance of research in developing a COVID-19 vaccine and the role of insurance for subjects in clinical trials. This is not what we would expect from a company that would deny insurance cover for adverse reactions post COVID-19 vaccine. Thus the claim by Salzone that refusal to cover is “verified by multiple sources”, in conjunction with the initial and consequent screenshot, appears to be disinformation. Insurance companies across Australia cover illnesses requiring hospitalisation following vaccination.
This leaves the obsession with claiming a 99% recovery rate as some type of stamp of insignificance. It is a rather tired trope having emerged about a year ago. This may also be linked to the frankly appalling claim that people die “with COVID, not of COVID”. Thus fatalities are incorrectly labelled an overestimation. Given this is pushed often by those who falsely insist vaccines kill and injure on a large scale it reflects a rather bizarre lack of compassion. As pointed out by USA Today the COVID-19 fatality rate is ten times that of influenza. More so it may be a serious diagnosis depending on age and health. To this we must add the emerging problems of ‘long haul’ symptoms perhaps in as many as 32% of those who have recovered from COVID-19.
In an interesting twist it was another wannabe COVID conspiracy-freedom-fighter who provided confirmation from Bupa that adverse reactions requiring hospitalisation are covered if their policy covers the treatment provided. It’s a bit of a story so another slide show is needed.
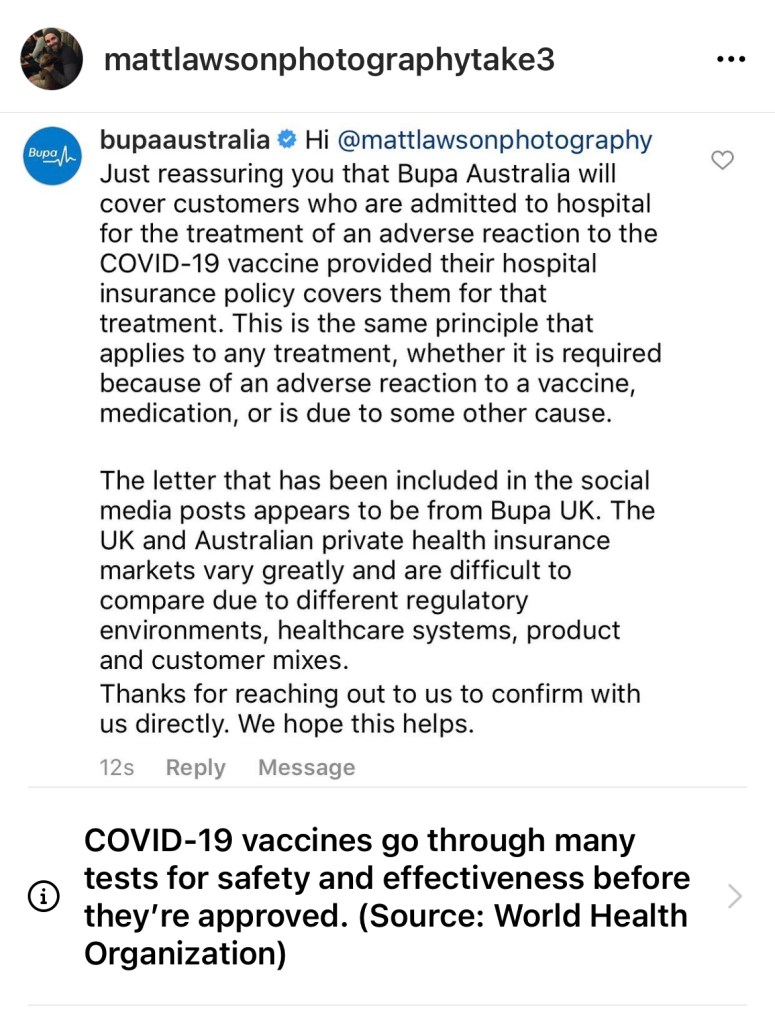
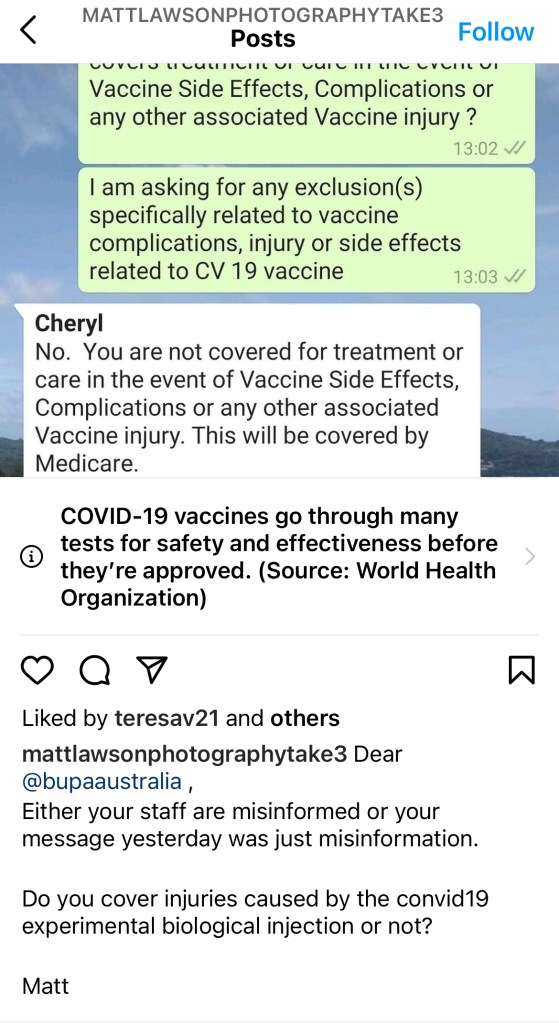
In the first image we see Bupa’s reply to anti-vaccine activist and COVID conspiracy theorist Matt Lawson, on social media. It outlines quite clearly that treatment covered by policy is available for adverse reactions post COVID-19 vaccination. In the next we see Lawson has engaged in a chat with ‘Cheryl’ from Bupa and presented this to Bupa on Instagram to challenge the prior response. The last screenshot was uploaded by Elle Salzone in the thread we’re discussing as another example of an insurance company denying cover to injury or reaction after COVID-19 vaccination.
Yet viewed in context we can see that during the chat Lawson supplied his policy number (image 3). So ‘Cheryl’ was answering in a specific sense, relative to his policy. This is absolutely in line with the claim made by Bupa in image 1 and also with feedback I’ve received from Bupa Australia. Still, image 2 reveals Lawson’s ill-informed, provocative reaction. The theme of acting with aggressive predetermined agendas is ingrained in the new age COVID conspiracy theorists. Matt Lawson reveals his conspiracy theory thinking when he writes;
Do you cover injuries caused by the convid19 experimental biological injection or not?
This comprehensive article reveals Bupa’s support for the COVID-19 vaccine and is in line with the position of global health authorities. There is no suggestion Bupa view the vaccine as experimental. Quite the opposite.
The letter mentioned in Lawson’s Instagram chat with Bupa Australia is circulating in social media within Australia. Within the Elle Salzone’s Facebook thread the image was uploaded twice, in support of the Allianz forgery. One commenter stated, “Another example shared of a void policy”. The second observed, “I think Bupa were one of the first…”. The image is below.
The text is as follows;
23 March 2021
Dear [redacted]
Thank you for speaking to me.
I confirm that side effects arising from the COVID-19 vaccine are not covered under our exclusion for: Complications from excluded or restricted conditions/treatment and experimental treatment exclusion.
If you are injured whilst doing COVID-19 swab yourself, cover would be available towards the injury.
I hope this information is helpful. If there is anything else we can help you with, please call our team on the above helpline number.
Yours sincerely
[signature]
Even if genuine, this letter has no impact on Australians. Peering at the Bupa letterhead we can confirm it is from Bupa Place in Salford Quays, Manchester U.K. Anti-vaccination activists will contend that the first paragraph confirms that side effects and complications from the COVID-19 vaccine are excluded from cover because it is an experimental treatment. The second paragraph conveys that insurance cover is available if one is injured, “whilst doing COVID-19 swab yourself”. In the U.K. home test kits are available.
Australians can also dismiss this as here it is illegal to advertise testing kits for serious infectious diseases. The TGA have a very clear warning to consumers and advertisers on their website. Thus there is no reason for Bupa to even consider such cover in Australia and Bupa members can disregard the letter and its claims.
Still, anti-vaccine claims are global in their reach, as is social media. If we take a cautious and in depth look into the origins of this letter there are different possible conclusions. It is a poorly written fake or a badly written follow up with a customer. Neither confirm the claim of an uninsurable experimental vaccine.
Bupa U.K. explain excluded and restricted cover in this Bupa Membership Guide [Archived]. This document provides a likely source for the information that the author presents with notably poor grammar. The opening paragraph is difficult to grasp. It may be that English is not the author’s first language.
With respect to the terminology used in the letter, on page 35 of the U.K. Bupa Membership Guide we find;
Exclusion 7 Complications from excluded conditions, treatment and experimental treatment
We do not pay any treatment costs, including any increased treatment costs, you incur because of complications caused by a disease, illness, injury or treatment for which cover has been excluded or restricted from your membership. […]
We do not pay any treatment costs you incur because of any complications arising or resulting from experimental treatment that you receive or for any subsequent treatment you may need as a result of you undergoing any experimental treatment.
On page 38 we find under Exclusion 16 Experimental Drugs and Treatment, this paragraph;
Please also see ‘Complications from excluded conditions/treatment and experimental treatment’ […]
There we have it. The text could have been copied and pasted in an extremely poor customer follow up, and that’s it above. Or copied and cobbled together in a dodgy forgery. The antivaccinationist lie of an uninsurable experimental vaccine is quite vocal on social media in the U.K. Yet under the glare of fact it is a demonstrably pointless effort.
In the U.K. COVID-19 vaccine side effects are covered under the Vaccine Damage Payments Scheme, established in 1979. This provides no-fault compensation for Adverse Events Following Immunisation. It is possible that offering cover is not an option for insurance companies. Either way, side effects are not covered by Bupa U.K. So it may well be that treatment of complications is classified as restricted and/or excluded regarding hospital cover.
The most important point here is that the COVID-19 vaccine is not an experimental treatment. Yet this letter is being pushed in Australian anti-vaccine circles to contend insurance companies are of the view it is experimental. Whilst a bogus claim, the overall forgery scam is reinforcing that claim in COVID conspiracy circles.
Bupa Australia are aware of this letter and have taken the chance to assure those who ask (such as the argumentative Matt Lawson) that cover is certainly available. When I raised this specific issue I was informed by Bupa Australia;
Private health care in the UK and Australia can vary greatly. But rest assured that our members will be covered for any hospital admission following an adverse reaction to the COVID vaccine, as long as the service is included in their cover, and any waits have been served.
Ultimately all the anti-vaccine points put forward by Elle Salzone and others on her Facebook page are demonstrably false. A search for insurance cover and COVID-19 vaccine adverse events yields results from around the world, not just Australia. For example cover for AEFI after the COVID-19 vaccine is available in Singapore whilst there’s a WHO compensation fund for people in developing nations suffering side effects. In general, insurance companies are involved in many areas specific to the COVID-19 vaccines, including in China where they are looking to cover adverse reactions.
Sadly some Facebook visitors to Elle Salzone’s page, who take her word on trust, are absolutely convinced of the dark side as this reply to me, packed with five pieces of misinformation, confirms. [Note – this is not from Salzone but a vulnerable visitor].
Sigh. Still all hope is not lost. As the well-known phrase from the X Files reminds us:
Last week AstraZeneca announced demonstrated varying efficacy in two different dosing regimens of its candidate COVID-19 vaccine, AZD1222 (ChAdOx1 nCOV-19).
In a November 23rd press release [PDF] the company announced efficacy of 90% when AZD1222 was given as a half dose and followed by a full dose at least one month later. This sample group had 2,741 subjects. Vaccine efficacy of 62% was evident when two full doses of AZD1222 were given at least one month apart. This was observed in a sample group of 8,895. They also announced a “combined efficacy” averaging 70% in a sample of 11,636.
Problems emerge
Whilst this sounded like a positive outcome it soon became apparent that the Oxford-AstraZeneca team still had hurdles to clear. It emerged later that the dose regimen yielding efficacy of 90% was given by mistake. This wasn’t made clear in the press release. The first dose should have been a full dose but due to a “manufacturing issue” only half of the expected dose was given. Regulators were told at the time and agreed the trial could continue with the immunisation of more volunteers. It is problematic that the trial wasn’t designed to test this regimen and less than 3,000 subjects aged 55 or less were involved. In order to validate the results another study examining the efficacy of the regimen will take place.
The other problem was the notion of “combined efficacy”. These data come from two different trials with different dosing regimens. One trial arm in the UK began in May. The Brazilian trial arm began in late June. So this information has not come from a single large Phase III trial as was the case with Pfizer and Moderna. Averaging efficacy from two different trials to yield “combined efficacy” of 70% is not acceptable. This doesn’t provide a sound assessment of what level of efficacy, or regimen, the public can expect. So again, further trials are needed. Also press release is not the vehicle to present scientific information and the AstraZeneca issue is an example of how problematic this can be. Study specifics that have been peer reviewed carry far more weight.
Media coverage
Which raises a point made by Norman Swan on today’s Coronacast that rumours are circulating, apparently with very little confirmation, that suggest Oxford-AstraZeneca are rushing to publish. He referred to a Financial times article which reported on Saturday;
Regulators and the rest of the world will soon have the full data. The Oxford academics who developed the vaccine have submitted a paper setting out their full Phase 3 results to The Lancet medical journal. They will be working over the weekend to answer questions from the journal and its referees and the article could be published as early as Thursday [UK time].
Concern and criticism about transparency and trust has been raised, particularly in the USA. Natalie E. Dean, assistant professor of biostatistics at the University of Florida posted a series of tweets on November 25th. Apart from transparency, concern about scientific rigour was raised. Her tweets included;
AstraZeneca/Oxford get a poor grade for transparency and rigor when it comes to the vaccine trial results they have reported. This is not like Pfizer or Moderna where we had the protocols in advance and a pre-specified primary analysis was reported.
The point about protocols in advance, along with the fact that AstraZeneca was one of nine vaccine makers to sign a scientific rigour pledge in September was raised in a highly critical article by Hilda Bastian writing in Wired. The article goes into the Phase III trial arms in depth and the manner in which Oxford-AstraZeneca has deviated from their trial protocol. Comparisons are made to the BioNTech-Pfizer vaccine at 90% efficacy and the Moderna vaccine at almost 95% efficacy. Bastian certainly casts them in a positive light. These two companies use messenger-RNA as the vector in their COVID-19 vaccines. Oxford-AstraZeneca use an adenovirus vector in their vaccine. How variously each approach effects COVID-19 vaccine efficacy is presently unknown. The Moderna and Pfizer vaccine results were also made public by press release.
It’s important to note that the FDA has argued a vaccine must be at least 50% effective to be useful in combating the pandemic. Whilst concern has been raised about the AstraZeneca situation it is over efficacy and not safety. The fact that regulators will accept an efficacy of at least 50% was noted by Mene Pangalos, AstraZeneca’s executive vice president for research, who dismissed concerns. AstraZeneca also want to alter the specifics of the US trial under the auspices of Operation Warp Speed. The aim is to change the two full dose regimen to a half dose, full dose regimen.
Certainly further successful trials are well within AstraZenecas grasp. The BMJ recently published COVID-19 vaccines: where are the data? The article examines the position of the three recent candidate vaccines and what is expected through peer-reviewed publication. The UK government has asked the Medicines and Healthcare products Regulatory Agency to evaluate authorising supply of the Oxford-AstraZeneca vaccine.
The cold chain needs of each vaccine vary. The Pfizer candidate requires storage at -70 degrees Celsius. This alone provides a challenge difficult to meet in developed nations and impossible in nations without significant infrastructure. Moderna’s candidate vaccine can be stored at -20 degrees Celsius meeting most pharmacy and hospital freezer temperatures but providing transport challenges for developing nations. Moderna claims that after thawing the vaccine will remain stable for up to 30 days at 2 – 8 degrees Celsius. AstraZenecas candidate can be stored in a normal refrigerator at 2 – 8 degrees Celsius and thus meets conditions in present healthcare settings and realistic options in developing nations. A successful outcome for Oxford-AstraZeneca is significant for the management of a global pandemic.
And remember, this is a vaccine that they promised not to make profits out of, that is cheap and they are committed to giving very large doses, I think something enormous like a third of the world’s doses of vaccines are relying on AstraZeneca. So there’s a lot riding on this vaccine.
Anti-vaccination lobby
The anti-vaccination community have taken the challenges faced by AstraZeneca as more evidence Big Pharma is always up to no good. A recent AVN Facebook post observed that maybe it wasn’t a good idea to let drug companies release their own study information without independent oversight.
So again we might consult the press release. It includes (para 3);
An independent Data Safety Monitoring Board determined that the analysis met its primary endpoint showing protection from COVID-19 occurring 14 days or more after receiving two doses of the vaccine. No serious safety events related to the vaccine have been confirmed. AZD1222 was well tolerated across both dosing regimens.
Our Directors are collectively responsible for the success of AstraZeneca. In addition, the Non-Executive Directors are responsible for exercising independent and objective judgement and for scrutinising and challenging management.
Quickly scattering the seeds of disinformation in this manner is what the AVN always do. One expects this manipulation of their members. What I’m more interested in is the inability of the group to acknowledge that the focus on COVID-19 vaccine development has revealed a number of long standing claims to be false. In September I posted on how the Oxford-AstraZeneca trial pause alone refuted long standing anti-vaccine claims. Namely transparent mainstream media coverage and the documented process of Phase III trials. Despite the ample criticism of AstraZeneca’s handling of data the AVN are even further from defending their claims than they were in September.
As a quick reminder it is the claim that vaccine manufacturers do not assess the safety or efficacy of vaccines. Ever. Added to this is the strange insistence that a placebo must always be inert. Let’s revisit quotes promoting these errors. Given that the COVID-19 candidates are new vaccines the following quote published in a response to a journalist is particularly relevant. See Proposition 4;
…there have never been double-blind, placebo-controlled prospective studies done on either the safety or efficacy of vaccines, not even when a new vaccine is introduced.
This piece on HPV is highly misleading. Yet it’s the claim in the second paragraph under Safety In Question I find compelling;
By definition, a placebo must be a totally inert substance which will never provoke a response.
That definition might be fine for the “sugar pill” placebo. As in when we think of the “placebo effect”. Yet in vaccine trials it is more important to sustain the double blind nature of the trial. Simply put a subject must not know what group they are in. The AVN are anti-HPV vaccination. Gardasil trials have used the amorphous aluminium hydroxyphosphate sulphate adjuvant, or AAHS as placebo. This, unlike saline, produces an injection site effect like a genuine vaccine. Thus members of the placebo group and those administering the dose are unaware they have received or given the placebo. The randomised double blind nature of the trial is preserved.
Double blind randomised control trials are what Meryl Dorey, founder of the AVN calls “the gold standard” insisting they are ignored in vaccine research. The claim is part of the AVN Did You Know? leaflet. In this case demanding only inert placebos be used helps to both refute the value of trials and contend a heavy metal neurological injury is potentially caused by adjuvant placebos. The impact of this rhetoric can be seen below in an image of an interviewee on the Vaxxed II bus (27 Nov. 2020). Her T-Shirt has the words “gold standard science” and “inert saline placebos” amongst others written on it in Texta.
Finally as discussed in this article, by contending that no vaccine trials using saline placebos have ever been conducted the insistence that vaccines are primed to harm persists. It’s a simple no true Scotsman anti-vaccine fallacy. Also when saline is used as the placebo in an HPV vaccine trial, there really is nowhere to hide. Vaccine studies using saline placebos abound. Period.
As it happens saline has been used in the USA arm of the AstraZeneca Phase III trials. In other groups a meningococcal vaccine is given as placebo. This won’t only create an injection site effect but a general feeling in line with being vaccinated. Not being aware they are receiving a placebo ensures subjects don’t introduce an unexpected variable to the trial. This fact, and the ethical nature of the approach is discussed in a well written article here. Finally in establishing the safety of vaccines a more convincing and in depth picture is gained through the application of more than just placebo controlled studies.
Conclusion
The more we see of Phase III trials for COVID-19 candidates, whether they be immediately accepted or controversial, the greater the refutation of the above anti-vaccine tropes. Senior members of the AVN are reading material that describes Phase III trials and their testing of both safety and efficacy. The above claim that double blind, placebo controlled trials don’t exist, “even when a new vaccine is introduced” still exists on the AVN website and in discussion. In the bright light of facts this is a true measure of the group.
The Oxford-AstraZeneca AZD1222 results have been met, understandably, with specific criticism. This relates to efficacy only. Safety is not being questioned. Some media reports have hinted that AstraZeneca will have difficulty getting the vaccine regulated for emergency use in the USA based on present data. Further, larger studies are needed to establish the veracity of the 90% efficacy finding in the smaller sample given a half dose followed by a full dose. This is entirely within reach of AstraZeneca.
Given the unscientific notion of a “combined efficacy” of 70% it is within AstraZeneca’s interests to pursue further research. Indeed everything being equal one may hope that the “combined efficacy” rate is not reinforced with further research. As STAT reported;
If it’s 70%, then we’ve got a dilemma,” said Fauci. “Because what are you going to do with the 70% when you’ve got two [vaccines] that are 95%? Who are you going to give a vaccine like that to?
AstraZeneca’s AZD1222 vaccine has enormous potential. The low cost, cold chain specifics and the company’s offer to not profit from the vaccine meets a global imperative for pandemic recovery. What the scientific community and the public need to see is a large robust Phase III trial that reproduces efficacy in the region of 90%.