Recently there has been some press coverage that potential running mates for Robert F. Kennedy Jr., are themselves well versed in conspiracy theories.
Kennedy, the driving force behind anti-vaccine pressure group Children’s Health Defense, which includes Children’s Health Defense Australia (recently abandoned website), is running as an independent for President of the USA. One possible running mate is Jesse Ventura who was mentioned here when the antics of Rima Laibow were reviewed. The other is Aaron Rodgers who has entertained a number of conspiracy theories including denial of the Sandy Hook shootings. Both are anti-vaxxers.
Kennedy has lobbied for years promoting the debunked link between MMR vaccines and autism. In the early days of the COVID pandemic he emerged as a vocal critic of COVID-19 vaccines. Which for a presidential contender, is understandably proving to be a problem. As measles cases rise across the US it isn’t surprising that Kennedy is not attacking vaccines on the campaign trail. In April last year Kennedy announced he would take leave of his roles as Chairman and Chief Legal Counsel of CHD, although the US site still lists him as both.
Exactly why the CHD Australian chapter URL is parked, just seven months after launching is unclear, although the Instagram page remains. What can’t be denied is Kennedy’s long history of spreading vaccine disinformation. In the early days of his campaign Kennedy talked about plans to tell NIH scientists it is time “to give infectious disease a break for about eight years”. However as his presidential campaign continues he is, according to NBC in the below clip, keeping his usual anti-vaccine message “relatively quiet”.
RFK Jr. relatively quiet on antivax message despite past ties
Critical overdose events at three Australian dance parties in January this year, have led to more calls for Pill Testing (PT) to be introduced as part of our nation’s effective Harm Minimisation drug policy. Harm Minimisation consists of three prongs: Demand Reduction, Supply Reduction and Harm Reduction.
Strong evidence
Pill testing is an evidence-based, harm reduction initiative backed in peer reviewed literature. It reduces drug harms and protects the health of those who access the service. Whilst Australian drug markets are uniquely sourced and specifically affect Australians, Harm Reduction Australia cites Harm Reduction International, in answering the question, What is harm reduction?
Harm reduction refers to policies, programmes and practices that aim to minimise negative health, social and legal impacts associated with drug use, drug policies and drug laws. Harm reduction is grounded in justice and human rights. It focuses on positive change and on working with people without judgement, coercion, discrimination, or requiring that they stop using drugs as a precondition of support.
PT has been demonstrated via live trials at Canberra’s Groovin The Moo festival in 2018 and 2019, to be effective in positively changing behaviour related to drug use. The trials were conducted by Pill Testing Australia, and resulting evidence greatly contributed to the fixed-site testing facility CanTEST, an ongoing trial in Canberra, introduced in July 2022. Indicating the controversy of PT, days before a third dance festival trial was scheduled to begin in 2022, Pill Testing Australia had public liability insurance withdrawn, without explanation.
A 2019 election study found two thirds of Australians support PT at music festivals. Examining deaths, PT initiatives, the success of harm reduction and drug user responses, Andrew Groves wrote in The Harm Reduction Journal in 2018:
Using a theoretical frame of pragmatism and drawing from national and international research evidence, this paper recommends the integration of pill testing into Australia’s harm minimisation strategy.
Australia’s Alcohol and Drug Foundation have published an excellent summary of the evidence supporting PT, and provide data on its successful international uptake. They also point out that public health experts have demonstrated support for PT. These include:
In February 2023, directly citing the success in Canberra, the QLD Palaszczuk government announced plans to develop Drug Checking at fixed and mobile sites. This very shortly followed the state’s plans to reduce penalties for illicit drug possession, including heroin, ice and cocaine. More so, use of the term “drug-checking” is more realistic, inclusive and in line with international practice, as summed up in this opening paragraph from the QLD Network of Alcohol and other Drug Agencies (QNADA):
Drug checking – also sometimes referred to as ‘pill testing’ – involves members of the public voluntarily providing samples of suspected illicit substances they are intending to consume (e.g. tablets, capsules, powders, tabs/blotter paper etc) for chemical analysis.
Test results are provided back to the individual by health professionals as part of a personalised health and harm reduction intervention. The purpose of the intervention is to increase the person’s awareness of the risks associated with the substance with the aim of effecting behaviour changes that result in fewer harms or incidences of drug-related death.
In September last year the QLD government sought private providers to offer plans for two fixed drug-checking sites and mobile services. Of course, great strides like this rarely escape unhelpful politicisation. It was impossible to miss that when announced, the decision was called “soft on drugs” by QLD opposition health spokeswoman, and registered nurse, Ros Bates. It’s been a long time since I’ve heard that phrase used seriously.
Victoria
It is Victoria, to where we must turn our attention to partly examine the recent overdose events. RACGP reported eight people, most in their 20s were intubated and placed in induced comas after MDMA overdose at the Hardmission dance party in early January. Jollyon Attwooll reported:
Chair of RACGP Specific Interests Addiction Medicine Dr Hester Wilson described the introduction of festival pill testing as ‘a no-brainer’. ‘[Pill testing] actually does change people’s behaviour, and therefore it makes it safer,’ she told newsGP. Dr Wilson said that pill testing is ‘not a silver bullet’ but should be used as part of a range of measures to address drug use.
Following the Hardmission OD events, two women were taken to hospital on January 12 after suspected drug use at Juicy Fest. Current Victorian Premier Jacinta Allan initially stated she had no plans to introduce PT. Not long after, Allan advised that she would seek more information from the health department. The Premier sensibly observed:
I think it’s important to examine the evidence and advice and consider that in the policy setting that we have across all of our alcohol and drug policy measures, which is taking a harm minimisation approach, looking at the safety of people going to events.
The ACT
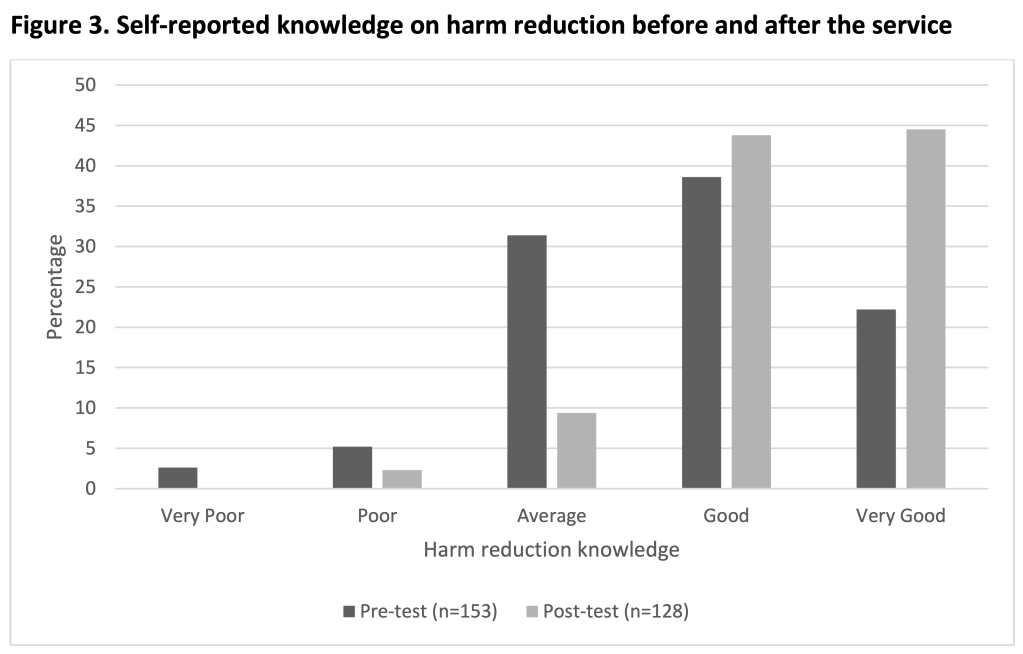
The evaluation document of the 2019 ACT Pill Testing trial is a lengthy read, with confirmation of Dr. Hester Wilson’s words coming through in data and discussion. I won’t copy/paste quotes from patrons who attended the PT facility, but I do recommend skimming through to appreciate that PT, like other harm reduction initiatives, changes drug users behaviour for the better. I did appreciate the graphs on self-reported knowledge of harm reduction before and after having a drug tested. Likewise, when it came to choice of information source, positive changes are evident.
Detailed explanation of the slides below can be found at section/s 6.1 (fig. 1), 6.4.1. (fig. 3) and 6.4.5. (fig.4).
Sydney
At the end of January a challenging scenario unfolded at Sydney’s HTID festival. Having taken what he thought was MDMA, an attendee fell unwell. Ultimately he responded to naloxone, a drug that reverses the effect of opioids. He had taken a tablet cut with nitazene, which is a synthetic opioid reported as “stronger than” fentanyl or heroin. Health workers and members of drug safety volunteers DanceWize, worked to advise the crowd. No doubt they saved lives. It turned out others from around Sydney had been hospitalised that weekend. One pill analysed, contained nitazene and no MDMA. Guardian reported:
Chris Gough, chief executive of the nation’s only pill testing venue in Canberra, said the detection of nitazenes in pills sold as MDMA showed the need for similar services in other states.
“In this case, where a nitazene has been sold as MDMA and therefore people are completely unprepared and potentially opioid naive, the risk of overdose is extreme,” said Gough, who is the executive director of the Canberra Alliance for Harm Minimisation and Advocacy.
“As we have now seen nitazenes in several jurisdictions in Australia it is time to act swiftly to provide drug-checking services throughout Australia so that we can respond to these drug trends as they emerge and thereby save lives and inform the community.”
Canberra
Saving lives is far more about probability than possibility. Indeed that’s been the case with MDMA overdose, MDMA pills cut with N-ethylpentalone or other adulterants. Early last year the Canberra walk-in site CanTEST discovered a pill cut with metonitazene; a synthetic opioid with a potency up to 200 times that of morphine. The owner chose to dispose of the drug on site. In January this year, ANU chemists made an Australia-first discovery of three new recreational drugs. All came from preparations sold as something else. CanTEST staff were able to discern the drugs were not what they were supposed to be, but tests were inconclusive. They were however, able to warn the community. One substance thought to be a derivative of Ritalin was in fact a new variant of cathinone, commonly known as “bath-salts”.
ACT Health have also developed a comprehensive document for festival planners. The Festivals Pill Testing Policy, examines PT options as a service available for festival attendees and how it relates to harm minimisation. Advice on general and specific health and safety measures, the importance of peer support, relaxation areas, emergency services and how PT works with providers and the event itself, is only part of the clear information presented.
Coronial support
A number of fatalities, and the fact that PT promotes positive decision making led to multiple calls to introduce the practice as a policy initiative. Over the last six years, four state coroners have spoken out. A 2020 inquest into five deaths from July 2016 to January 2017, led Victorian coroner Pares Spanos to urge the Victorian government to “urgently” introduce drug checking and a system to warn the community about dangerous substances sold as MDMA. The males aged from 17 to 32 died in a variety of tragic ways after taking what they believed was a modest dose of MDMA. Autopsy revealed the substances 25C-NBOMe and 4-Fluoroamphetamine in their systems. The cluster was discovered after 20 hospitalisations stemming from the Chapel Street nightclub district in January 2017. Victoria Police knew of the dangerous drug’s presence and later defended their decision to not warn the community.
In September last year, Victorian coroner John Cain also called on the government to introduce PT after the death of a man from an MDMA overdose in March 2022. The man had been observed taking a Blue Punisher, a pill with dangerously high levels of MDMA. He was admitted to the Royal Melbourne with brain swelling and multi-organ failure and died four days later. In his findings Cain wrote:
It is impossible to know whether, had a drug checking service existed, [the man] would have submitted a sample of an MDMA pill for testing before taking it at Karnival […] Notwithstanding this, a drug-checking service would have at least created the opportunity for him to do so, and for him to receive tailored harm reduction information from the drug-checking facility.
It is likewise impossible to know whether, had [the man] been provided information of this type, he would have changed his drug consumption behaviour; but likewise, in the absence of a drug checking service, this was not a possible outcome.
Politics
NSW and Victoria have established histories of resisting PT. After the death of a 26 year old at a Sydney music festival in February 2023, Dominic Perrottet mused about his government’s inquiry into methamphetamine and, rejecting any notion of PT offered a most unhelpful contribution:
But my clear message to people right across NSW [is] stay safe, and don’t take drugs and you will be safe.
Associate Professor David Caldicott, one of the driving minds behind CanTEST, suggested Perrottet had engaged in “magical thinking”. In Victoria we have the legacy of Dan Andrews who, citing the demonstrably false [HRJ] claim that PT encouraged pill taking (a belief favoured by Craig Kelly), insisted that under his leadership PT would never be introduced. The state opposition has been steadily opposed to harm reduction measures for conservative political reasons. Ignoring evidence, consecutive opposition leaders have opposed Safe Injecting Facilities and PT alike. I do acknowledge however, that the Victorian opposition has lobbied the state government for more effective emergency drug alert systems.
Recent research
A recent paper Drug-related deaths at Australian music festivals, was published last month in the International Journal of Drug Policy. Examination of the National Coronial Information System (NCIS) yielded the following results about fatalities at music festivals between 2000 and 2019:
There were 64 deaths, of which most involved males (73.4%) aged in their mid-20s (range 15-50 years). Drug toxicity was the most common primary cause of death (46.9%) followed by external injuries (37.5%). The drug most commonly detected or reported as being used was MDMA (65.6%), followed by alcohol (46.9%) and cannabis (17.2%), with most cases reporting the use of two or more drugs (including alcohol) and 36% reporting a history of drug misuse in the coroner’s findings. Most deaths were unintentional, with less than a fifth of cases (17.2%) involving intentional self-harm. Clinical intervention was involved in 64.1% of cases and most festivals occurred in inner city locations (59.4%).
There are complex factors identified in the paper, such as inner city events and multi-day events being more likely to be the site of a fatality. This may reflect policing strategies and the need for harm reduction strategies, respectively. Alcohol is known to be a compounding factor and its use is clearly identified as the second most prevalent substance (see bar graph below). Males are more likely to drink and use MDMA and this is reflected in them making up just under three quarters of deaths. Of 2000 festival goers surveyed, 52% were male. Poor decision making associated with alcohol intake is always a potential factor with illicit drug use.
Total number of drug-related deaths, deaths primarily attributed to MDMA, and deaths primarily attributed to alcohol, at music festivals in Australia by year ranges (n=64)
Harm reduction flexibility
What I took away from this paper was the recommendation that a range of harm reduction measures would each have something to offer in solving this persistent, multifactorial problem. More so, understanding data yielded by such research is vital to establishing the correct harm reduction approach for the Australian population in these instances. In conclusion, the authors write:
Harm reduction strategies such as roving first aid volunteers, mobile medical care, spaces to rest, hydration stations, and drug checking services, may best address some of the risks associated with illicit drug use at festivals, in addition to increased consumer education and awareness. It is important to understand the factors involved in these incidents in order to inform policies around harm reduction and law enforcement at music festivals in future to prevent further deaths.
Just as is the case with injecting facilities, substance checking is a successful, global health policy dynamic. Like all aspects of harm reduction the evidence supporting it is strong, persisting through variations specific to where it is a reality. In Canada, Toronto ran a comprehensive trial from 2019 to 2023. Switzerland has had drug checking available since the 1990’s. Now in a number of cities, the past decade saw a 250% increase in samples tested there. The UK has drug checking services, as does New Zealand.
Despite certain dynamics in NSW and Victoria leaving state governments out of touch with most Australians, there are cabinet ministers and cross-bench teams respectively, raising awareness and pushing for change in each state. When we look at arguments for and against PT, it appears arguments against, lack realistic substance. Indeed these documents recognise the importance of harm minimisation and its place in the National Drug Strategy. The most comprehensive argument “against” is criticism of the limitations of on-site drug checking, compared to laboratory testing. This is well understood and has been directly addressed by Dr. Monica Barratt. Of course the inevitable case that flexible harm reduction measures encourage or create the illusion of safety around illicit drugs is always mentioned. The evidence simply does not support this.
Drug Free Australia
This brings us to the anti-drug lobby. Certain groups contend that law enforcement and zero tolerance are superior in managing drug related harms. Stridently anti Harm Minimisation, they promote the ideology of a drug free world, consistently undermining evidence. In fact my own interest in the anti-vaccination lobby, began in 2009 and I was struck by similarities between their tactics, and those of the more lethal anti-drug lobby, I was long familiar with.
One group, Drug Free Australia (DFA), operate similarly to The Australian Vaccination-risks Network (AVN). DFA aggressively lobby government and an unsuspecting public, frequently using alarming irrelevant information. They attack the media, use meaningless or decontextualised data to dispute published evidence or argue that acknowledging a need for more research, reveals lack of any research. DFA dismiss harm reduction techniques by highlighting the ongoing presence of harm (eg; MDMA has caused deaths, thus no rationale for PT exists) or blame harm reduction for drug user risk-taking, and the familiar contention that PT “green lights” the taking of MDMA.
Such contentions stem from ignoring that high risk behaviour via illicit drug use continues all day, every day in Australia. Harm reduction aims to reduce the harms associated with this behaviour. It provides education, promotes safe choices, saves our health-system money, and yes, saves lives. One way DFA contend PT actually kills, is by misrepresenting the PT card system. A drug found to contain what the owner expected is “white-carded”; as is say, an MDMA pill free of any pollutant. Yet, MDMA causes most overdoses say DFA, so a white-card result must be potentially lethal. Well, no. The drug is what the person expected. Not double or five times the amount. So the patron may take the drug they bought and, remembering the slide show above, will henceforth access reputable information on harm reduction.
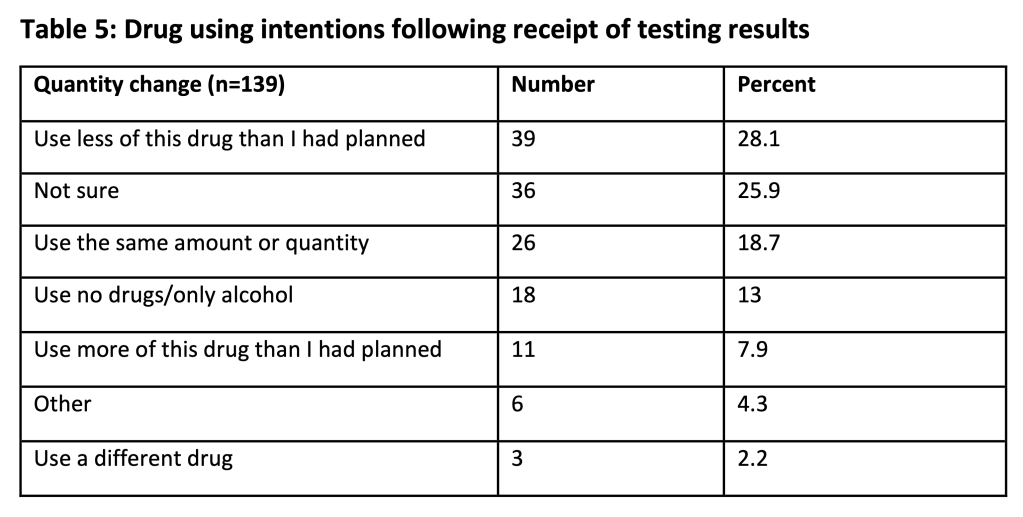
Those slides are from the ACT Pill Testing Trial 2019. DFA attack those findings in a deceptive piece, arguing the opposite to accepted findings. On page 7, they selectively quote from evaluators who discuss that someone who discovers that the drug is what they thought, “…are likely to take as much or more” (p.33). And that “…concordance between expectation and identification is associated with stable or increased intention to take a substance” (p.34). DFA use this to extrapolate to the conclusion that PT will lead to more use and thus, more death. This requires logical fallacies: Decontextualisation and cherry picking of data. Reading the full sentences and paragraphs in which those terms appear leaves the reader with a positive, not negative view of the evaluation. See pp. 33-34, and consider Table 5 from p. 32, below:
When read in context we see that patrons intent to use drugs did not dramatically change, but their intent to engage in harm reduction behaviour notably increased. Eg, also on p.33 (bold mine); Many interviewees reported that the quantity of drugs that they intended to use did not change after testing, as the drug was identified to be what they expected. And, Many interview patrons indicated that their intention to use did not change, but their intention to engage in harm reduction behaviours did increase. Also, this and other evaluations have found non-concordance between patrons’ expectation of what a substance is and what a substance is identified to be, commonly leads to reduced intention to take that substance.
So, the comment pulled from p. 33 by DFA, omits crucial clarification from the evaluation. Some was printed on the same page, just two paragraphs above. For example:
Interview data suggests that this group were looking for confirmation of the contents of the presented drug, and information about how to reduce potential harms. Many interview patrons indicated that their intention to use did not change, but their intention to engage in harm reduction behaviours increased.
Prior research also indicates concordance is associated with an increased likelihood of taking the drug, and non-concordance with a decreased likelihood (Valente: 2019, and Measham: 2018). More so, the evaluators stress that modification of drug consumption can’t be measured alone. Contextual factors, such as type of festival influencing available drugs, need to be considered during interpretation of results and future study design.
Finally, the insistence by DFA that MDMA, not impurities, lead to most fatal overdoses is fashioned only to discredit PT. Still, five deaths in the six months leading up to January 2017 and investigated by Coroner Pares Spanos involved 25C-NBOMe and 4-Fluoroamphetamine. Recent discovery of potent opioids nitazene and metonitazene raise further concern. N-ethylpentalone is regularly found in so-called MDMA pills. But why get hung up on MDMA? Drug checking can check any drugs and CanTEST discovered three unknown substances, later confirmed at ANU. This is how a new type of cathinone (bath salt) was found. Supposed ketamine was actually a new type of benzylpiperazine (BZP) stimulant. The third find was propylphenidine.
Conclusion
Pill testing or drug checking is a harm reduction measure supported by consistent evidence in peer reviewed literature. Globally, where introduced, it has demonstrated success and improved understanding of behaviour. It is supported by most Australians, where valuable data has been gathered from on-site testing at music festivals, and the fixed site CanTEST, in Canberra.
This has expanded the nation’s understanding of drug user insight into, and uptake of harm reduction dynamics. QLD is the most recent state to confirm permanent drug testing. Arguments against the initiative are morally subjective and/or deceptive, leading to their swift deconstruction.
Drug checking saves lives and is supported by public health experts across Australia. As a dynamic, expanding, harm reduction initiative, it should be introduced nation-wide into Australia’s harm minimisation strategy.
♠︎ ♠︎ ♠︎ ♠︎
Originally published as Pill Testing: The harm reduction initiative supported by strong evidence
Mal Vickers is a skeptical activist with a singular focus on shonky so-called treatments, and the much-to-be-desired responses of regulators responsible for keeping our community safe.
In 2016 Mal received the ‘Skeptic of the Year’ award, jointly with Dr Ken Harvey for complaints about chiropractors. While studying towards a Master of Public Health, Mal investigated the complementary medicines market using the complaints made about its advertising and products. Mal is a mild-mannered bio-medical engineer and enjoys photography and tinkering in his workshop.
Working with Dr. Ken Harvey Mal has been instrumental in targeting false claims that can harm consumers. They reported on persistent non-evidence based claims in breach of the Chiropractic Board and AHPRA guidelines, and the absence of appropriate responses from these regulators.
Mal and Ken published the first review of the TGA’s Complaints Resolution Panel over its entire 19 year life. The analysis comprehensively demonstrated the failure of the TGA to ensure regulatory compliance by advertisers of complementary medicines.
While our regulatory system is meant to rein in violations, from 1999 to 2018 complaints and established breaches of the law greatly increased. At Skepticon, Mal will peel back the layers of misleading advertising that ultimately wastes people’s time and money.
How do the companies behind these products get away with it? And, who tops the list for unethical behaviour?
The COVID pandemic gave voice to a number of conspiracy theories that sought to offer an explanation about what was “really” happening. Some of the more bizarre, and yet persistent, conspiracies involve an inexplicable plan of global depopulation. Or as it is often labelled, “culling”.
A decade before the pandemic, anti-vaccine conspiracy theorists had accused Bill Gates of using vaccines in his own quest to depopulate the planet. That was an intentional distortion of a TED talk Gates had given in which he notes that improved public health correlated with decreased population growth. Over time it became a particularly robust piece of misinformation, commonly spread with the unfounded claim that vaccines cause infertility. Claims of vaccine induced depopulation and infertility found new ground during the pandemic. As the pandemic continued a host of conspiracy theories about vaccines were entertained by antivaxxers in a bizarre ebb and flow fashion modulated by social media.
Another identity associated with the depopulation conspiracy theory to be dusted off during the pandemic was psychiatrist, Dr. Rima Laibow. Rima was referenced on social media in 2021, January 2022 and most recently in March 2023. Laibow’s attraction was due to her appearance on the 2009 programmeConspiracy Theory with Jesse Ventura. Motivated by H1N1 (“Swineflu”), anti-vaccine conspiracy theory rhetoric, Laibow claimed during an interview that the World Health Organisation had been working since 1974 to orchestrate global depopulation. She claimed the WHO assessed the world overpopulated by 90% and was using vaccines to create “permanent sterility”. That the population had grown from 4 billion to just under 7 billion from 1974 to 2009 was seemingly lost on her.
April 2023 Instagram post from a now deleted account
Her 2009 appearance with Jesse Ventura was being shared on social media along with commentary suggesting that Laibow had “nailed it” and foreseen both mandatory vaccination and “the great culling“. In the histrionics of conspiracy theory echo chambers this was proof that the WHO was using COVID-19 vaccines to create permanent sterility, and that Laibow had “cautioned us against COVID-19”. It must be stressed that mandatory vaccination either for H1N1 or COVID-19 never eventuated. There has been ample controversy regarding vaccine mandates in certain workplaces during the COVID-19 pandemic, but in no way have Laibow’s claims been realised.
On 26 April 2022 Health Feedback published a fact check of another of Laibow’s accusations in the video. Namely, the claim that squalene in vaccines caused autoimmune disease and Gulf War Syndrome. Unsurprisingly, the verdict was “inaccurate”. Laibow warned of the horror vaccines would unleash, telling Jesse Ventura, “What that means is a genocidal holocaust. Men and women will sicken and die and those who survive will be infertile”. The YouTube video below contains the circulating clip of Rima Laibow, edited to educate the viewer as to Laibow’s relationship with science, the truth and legislation.
Dr. Rima Laibow
Selling Colloidal Silver
During her interview Laibow dramatically remains on the edge of a tarmac lest she need to suddenly escape from the USA to avoid “compulsory vaccination” for H1N1. She did not feel safe living in the USA and tells Ventura she was leaving as soon as the interview was over. However, it appears she managed to overcome her fear to work as “medical director” and trustee of the company, Natural Solutions Foundation, with a website hosted at drrimatruthreports.com. By 2014 Rima Laibow was selling a “cure” for Ebola. The “cure” was 10 PPM Nano Silver, which was in fact colloidal silver, and packaged as “Dr. Rima Recommends Nano Silver”. In September 2014 the US Food and Drug Administration and the Federal Trade Commission labelled the company “scammers”. A warning letter to the company informed Laibow and a co-trustee that they were in breach of the Federal Food, Drug and Cosmetic Act (FDCA).
The correspondence includes examples of strikingly inaccurate claims made on the Natural Solutions Foundation website in which nano silver is described as “safe and non toxic… able to kill every pathogen worldwide against which it has been tested”. Health authorities were of course hiding the truth of this cure and the absence of “declassified research” supporting colloidal silver was proof it is effective. Packaged with a CBD organic chocolate bar, nano silver constituted part of a “protection pack”. Other claims included:
Conventional Antibiotics won’t do much against genetically engineered or resistant organisms… But safe, gentle and effective nano silver kills disease organisms in a different way… This is powerful natural protection you need for yourself ad [sic] your family. Choose the Personal Protection Pack or the Family Protection Pack…
It kills only the organisms that cause disease… similar to the lamps in hospitals that kill deadly germs… and also interferes with the metabolism of the disease organisms in such a way that they cannot become resistant to it.
Laibow responded by altering claims made on the company website. The scheme was heavily criticised on the7 On Your Side TV programme “Don’t Get Taken By Ebola Scams”, in which Laibow reportedly argued the scam label was “ridiculous”. Ebola scams were common in the USA at the time, taking the form of bogus charities and cures. Ebola cases and deaths had occurred on US soil and scam artists were taking advantage of fear and uncertainty.
By 2020 of course, the pandemic was upon us. Did Rima Laibow actually turn to reminding us that she had warned of the WHO depopulation-by-sterilisation using vaccines? Did she flee the US in fear of mandatory vaccination? Well no, because Natural Solutions Foundation immediately got to work selling the very same Nano Silver concoction as a treatment for COVID-19. At the same time COVID conspiracy theories were peddled via the long standing Dr. Rima Truth Reports, and went as far as calling face masks “mind control devices”.
Ultimately, the FDA filed a suit on 13 November 2020 that alleged Natural Solutions Foundation, and its trustees Rima Laibow and Ralph Fucetola, had “sold and distributed a nano silver product that the defendants claim will cure, mitigate, treat, or prevent COVID-19.” It further alleged that they had sold misbranded drugs, as labelling for use was insufficient. As such they had violated the FDCA, and on 28 December 2021 were ordered by a District court to stop distributing the colloidal silver. This was the same product used in breach of the same Act as in 2014, albeit now in exploitation of COVID-19.
‘Dr. Rima Recommends’ nano silver label
Fortunately, this time the outcome was more enduring. The defendants agreed to settle the suit and be bound by a Consent Decree of Permanent Injunction [PDF]. The court entered an order that enjoins the defendants from violating the FDCA. They were ordered to recall all nano silver products sold from 22 January 2020 to 27 December 2021, and destroy any such products in their possession. Before distribution of any drugs in future they must notify the FDA in advance, comply with remedial measures and permit an FDA inspection of their facility and procedures. On 8 March 2023 the FDA published an urgent product recall from the company for the nano silver product, issued as part of the consent decree.
These days Dr. Rima Laibow and Ralph Fucetola of Natural Solutions appear on Open Source Truth [archive] and present a weekly podcast titled The Unmasked Crusaders. The Natural Solutions Foundation website is unchanged from a decade ago and the Dr. Rima Truth Reports continue. They do not, thankfully, sell colloidal silver.
The anti-vaccine, anti-mask, anti-science rhetoric however, is undiminished.
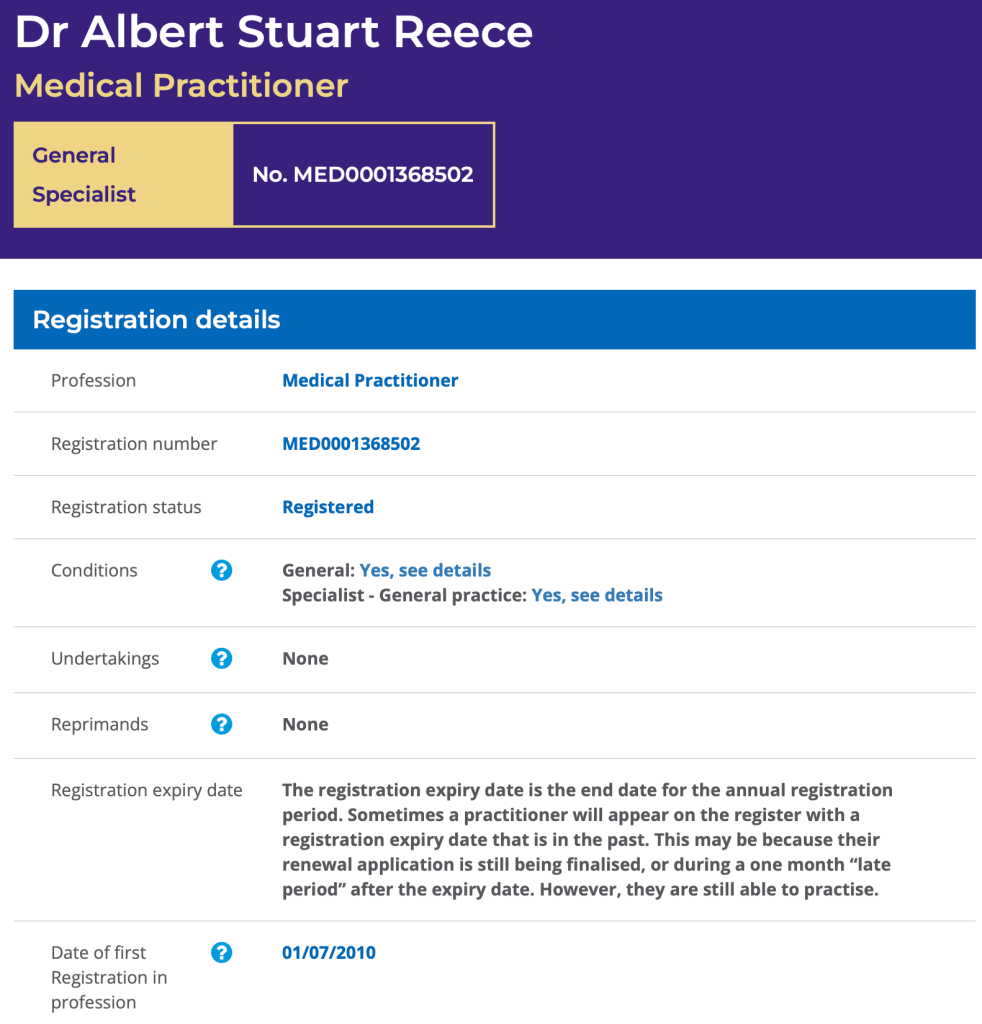
The Medical Board of Australia has placed fifteen limitations on the practice of Dr. Stuart Reece of Highgate Hill QLD. The conditions, enforced on 21 December 2022, have resulted in the temporary closure of the Southcity Medical Centre where Reece practices.
Reece (pictured) is a controversial figure in addiction medicine and a vocal critic of Australia’s successful policy of harm minimisation. He holds no formal qualifications in addiction medicine, but has authored or coauthored extensively on the subject, presently as an adjunct professor at UWA. Almost exclusively, his writings link illicit drug use, methadone and medical cannabis to death and disease.
Experts have refuted certain works as “reefer madness”. Reece has long associated his Christian faith with treating addiction. His book, titled “Let My People Go: A Theology of Addiction”, was published in 2016. His work is favoured by extreme anti-drug pressure group, Drug Free Australia, and frequently cited by them in lobbyist material, media replies and parliamentary submissions.
This is not the first time regulators have acted to ensure the safety of his patients. An article published on this blog in December 2011 examined his use of unapproved naltrexone implants and the deaths of 25 patients who had undergone the treatment. In 2009 Reece was suspended from practice for supplying morphine to opiate dependent patients and falsifying records to disguise the fact. This was because of his ideological opposition to evidence backed methadone maintenance therapy. That suspension was in turn suspended for three years.
The Medical Board of QLD, Health Practitioners Tribunal observed at the time that Reece:
… has a somewhat evangelical approach to this area of medicine and because of that he does appear to lack a degree of insight and objectivity in relation to the treatment of his patients. Furthermore, he seems to feel that the ends justify the means in terms of treatment of patients.
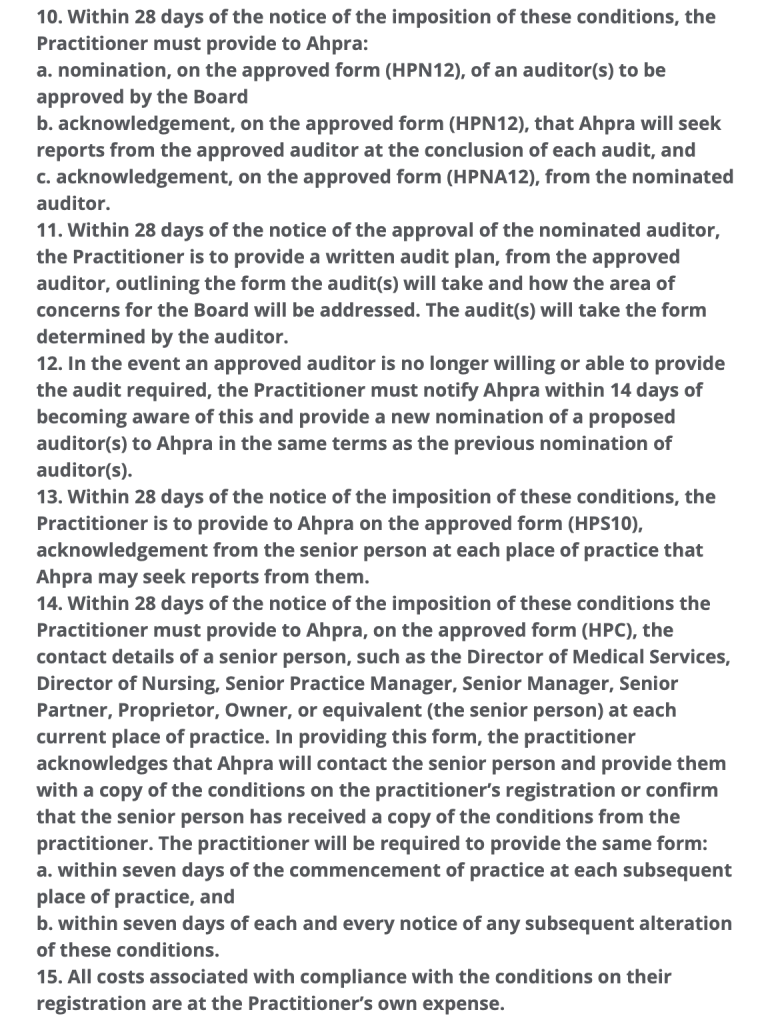
Today, the catalyst for intervention includes the number of patients being bulk billed per hour and quality of care. This is reflected in the limitations on practice (complete list in slideshow below).
1. The Practitioner must not exceed four (4) of patient consultations in any one hour (60 minutes). […]
5. The Practitioner must only practise as a general practitioner when supervised by another registered medical practitioner with knowledge and experience in addiction medicine (the supervisor). For the purposes of this condition, ‘supervised’ is defined as: The Practitioner must consult with the supervisor who is always physically present in the workplace and available to observe and discuss the management of patients and/or performance of the Practitioner when necessary and otherwise at weekly intervals. […]
7. In the event that no approved supervisor is willing or able to provide the supervision required the Practitioner must cease practice immediately and must not resume practice until a new supervisor has been nominated by the Practitioner and approved by the Board.
A search for general practitioners providing services in addiction medicine in the Brisbane area yields modest results. There just isn’t enough practitioners providing these select services across Australia. If one adds the fact that such providers have often taken on all the patients they can, it isn’t beyond comprehension that Dr. Reece is unable to find a supervisor. Reece has loyal supporters amongst his patients, who have a Facebook page here. They have argued in a petition that finding a supervisor is “an impossibility”. The petition, “Reinstate Dr. Stuart Reece Immediately”, contends that the predictable lack of a supervisor indicates that the action taken is about the control of services offered under bulk billing.
AHPRA is also advising that Dr Reece must have another Doctor with him for consultations into the future to oversee his work to their satisfaction. This requirement is an impossibility. AHPRA and Dr Reece both know that this doctor does not exist. There is not a ‘spare doctor’ lying around that is available for this. […]
THIS IS NOT ABOUT PATIENT CARE OR BETTER HEALTH OUTCOMES. THIS APPEARS TO BE ABOUT CONTROL OF THE TYPE OF SERVICES OFFERED TO PATIENTS WHO NEED BULK BILLED DOCTORS.
The petition is a long heartfelt plea seeking to justify the way Reece operates his practice. It makes the point that certain appointments, particularly prescription refills, may require only five minutes. The petition also notes that Reece would be forced to close his doors in part because, “his practice would be limited dramatically by the immediate reduction of the number of patients he is able to see daily…”. Whilst I empathise greatly with these patients and find removal of any addiction treatment services troubling, one cannot escape the fact that such a huge patient load should never have eventuated. Health Practitioner Regulations state, “A Practitioner must NOT exceed four (4) patient consultations in any one hour (60 minutes)”.
There’s no doubt that Medicare is not meeting the needs of Australian General Practitioners. The patient rebate is beyond inadequate, being markedly out of step with the Consumer Price Index (CPI). This manifests in significantly fewer consultations being bulk billed, and in many practices fees now apply to concession card holders. For Australians surviving on the aged or disability support pensions a visit to their GP is now financially prohibitive. The end result is a health system under strain. However there comes a point where increased patient quantity, means decreased quality of care. Let’s remember that the Health Practitioners Tribunal observed in 2009 that when it came to treating patients Reece lacked insight and objectivity, and felt the ends justified the means. The same document notes (point 22):
He does provide care to a large number of detoxifying and drug dependent patients. In June 2009, alone, he had 409 Subutex patients in Queensland and I understand the numbers are larger at the moment. From 2001 to 2007 he was responsible for 8681 registrations of opiate withdrawal registrations in Queensland.
Arguably, Reece is the architect of his own professional distress. As noted above, in November 2009 the practice suspension applied to Reece was itself suspended for three years. Yet less than two years later there was no tone of contrition for falsifying medical records to supply opioid dependent patients with morphine. The occasion was a Senate Inquiry into the Professional Services Review (PSR) Scheme, to which Reece, representing the now defunct Australian Doctors Union, made a submission. Bear in mind Reece has today been saddled with limitations to prevent excessive bulk billing at the expense of Medicare. The PSR “aims to protect the Australian public from the risks and costs associated with inappropriate practice within Medicare…”. Reece began his submission:
Prof. Reece: The Australian Doctors Union is a nascent union which has come together to support each other through the nightmare experience of PSR’s incompetence, lies, intimidation and bullying. In addition to doctors damaged by—
CHAIR: Hang on please. That is making accusations and it is not the way that we take evidence. If you could please refrain from using that sort of language, that would be appreciated.
Reece continued for a full five minutes explaining why he believes the PSR “has been shown to be waging a very successful war against general practice in this country”. He blamed the PSR for doctor suicides, marriage breakdowns, a lowered bulk billing rate, marginalisation of women, being racist, sexist and for damaging “many excellent doctors”. One of these was his ideological colleague, “Dr George O’Neil of naltrexone implant and detox fame”. Despite the fact naltrexone implants are not TGA approved Reece felt O’Neil should have been assisted by Medicare. Perhaps most alarming was when Reece included himself as one of those excellent doctors. Referring to himself in the third person, he humbly submitted:
Associate Professor Stuart Reece, one of the foremost detox doctors in the nation and a world authority on the long-term effects of opiate addiction.
This dear reader, is the crux of the matter. Stuart Reece is not a world authority on the long term effects of opiate addiction. In 2007 he opposed needle-syringe programmes, methadone maintenance therapy and the policy of harm minimisation in general. He informed a parliamentary inquiry that condom use was linked to AIDS deaths. Yet in June 2009 Reece was managing 409 Subutex patients. Buprenorphine is the opioid in Subutex and today it is distributed in combination with naloxone under the brand name Suboxone. It is a successful mainstay of substitution therapy for opioid dependent patients seeking to manage addiction and eventually cease opioid use. It is a key element of harm minimisation.
Exactly how a strident opponent of harm minimisation has today found himself with so many opioid substitution patients that Ahpra require supervision and auditing of him, is baffling. It may however have something to do with the attitude toward Medicare and the PSR Scheme reflected in his 2009 submission. Or his 2012 comment, What is wrong with medicare? (p. 170) bemoaning the PSR and Medicare audits. It may also have something to do with the disdain Reece has for evidence based health policy and genuine, original research. Reece has spent a career convinced he simply knows better. Better than the bulk of his colleagues, better than global research trends and better than health authorities. In short, Stuart Reece is the cause of the dilemma faced by so many of his patients.
Having said that, one cannot deny that Reece and Southcity Medical Centre have been accomodating the needs of a great many patients. An excessive number of patients. However accounts such as this on reddit aren’t isolated. They suggest the practice is busy, waiting times are high but Reece is attentive and compassionate. Google reviews are more varied. According to the petition there are 1100 patients in need of treatment. Over the last 18 days, 224 people have signed. The goal is presently 500.
Ultimately this situation doesn’t bode well for these patients. It is doubly sad that many are not able to see that the cause of their problem is Stuart Reece himself and not Ahpra. Funnelling high numbers of vulnerable in-need, at-risk patients through the surgery is far from acceptable. The only way forward is to abide by the limitations. Anything less is to abandon his patients.
Stuart Reece must accept that the ends do not justify the means. It is time to place patients first.
Medical Board of Australia restrictions imposed on Dr. Stuart Reece