The Therapeutic Goods Administration (TGA) is aware of misinformation in recent media and online reports that claim the COVID-19 mRNA vaccines are contaminated with excessive levels of DNA. This is not the case.
So opens the TGA report Addressing misinformation about excessive DNA in the mRNA vaccines. It is, for those of us aware of this issue, an understatement. The sheer volume and scope of misinformation, combined with relentless pressure from repeat offenders including members of the Australian parliament, more accurately suggests a campaign. A calculated campaign of misinformation designed to spread fear and intimidate the vaccine hesitant. Despite there being accepted means for discerning DNA residue in vaccines, two claims persist. Namely levels are hundreds of times greater than the accepted safe level, and that aggressive cancers will, and do, directly result.
Background
The original claim stems from a preprint paper by Kevin McKernan dated 11 April 2023. Amplitude, via the Australian anti-COVID vaccine lobby, was lent to this claim in July 2023. The legal guru behind all Australian court cases to challenge approval of COVID-19 vaccines, retired barrister Julian Gillespie, penned The Canaries in the Human DNA Mine. Falsely labelled “peer reviewed” by his anti-vaccine compatriots, it was published in the unabashedly anti-vaccine International Journal of Vaccine Theory, Practice, and Research. Gillespie also crafted the case material used by Dr. Julian Fidge, in what became known as the Fidge v Pfizer case in which Fidge was represented by Katie Ashby-Koppens of P. J. O’Brien and Associates. I summarised the unsuccessful case here, in April this year. Gillespie and Co. followed with a conspiratorial constitutional complaint against the presiding judge, Justice Helen Rofe. Then via a High Court writ they targeted Chief Justice Debra Mortimer for not accepting their complaint. Both complaints were lodged on behalf of Dr. Fidge
Around the same time, the outrage manufactured by the anti-vax lobby shifted from the claim in Fidge v Pfizer that mRNA vaccines were Genetically Modified Organisms (GMOs), to the claim that vast amounts of DNA were contaminating these vaccines. Julian Gillespie, who wants a COVID Royal Commission, publishes for his “good substack folk” regularly on DNA contamination. He claims to have commissioned Canadian molecular virologist Dr. David Speicher to pursue said contamination, ultimately announcing confirmation on 6 June. Speicher was not a surprise choice for Gillespie. He had published with McKernan, Jessica Rose, Maria Gutschi, and David Wiseman in Canada in October 2023, reaching the contamination conclusions Gillespie wants to hear about.
It bears stressing that Kevin McKernan’s preprints lost credibility long ago, when it became apparent the vials he tested were of unknown origin. More so, if origin is unknown then cold chain transport requirements are by default, breached. In October 2023, David Gorski referred to McKernan’s initial preprint as an “awful study” and follow up studies being “equally as bad”. Thus it is unsurprising further attempts were made to label COVID vaccines as DNA contaminated. The Global Vaccine Data Network provide an excellent refutation of what they call Plasmid-Gate. As a highly COVID-19 vaccinated nation, Australia is used in their piece as an example to debunk the claim of so-called “turbo cancers” resulting from COVID-19 vaccination. SBS recently reported that last year, biologist Phillip Buckhaults from the University of South Carolina spoke before a state panel postulating the possible consequences of DNA contamination. When his comments took flight on social media he quickly followed up on X with insistence that such a risk was “purely theoretical”. They further reported that:
Dr Paul Offit of the Children’s Hospital of Philadelphia said [DNA] fragments were “clinically and utterly harmless”.
“These DNA fragments would have to enter the cytoplasm, which is that part of the cell outside of the nucleus, and our cytoplasm hates foreign DNA,” Offit said. “It has innate immune mechanisms as well as enzymes to destroy foreign DNA.”
Also interested in supposed DNA contamination of mRNA vaccines are Senators Malcolm Roberts, Gerard Rennick, Ralph Babet, Alex Antic and Russell Broadbent. Rennick has pushed both the GMO and DNA contamination angle for well over a year. Broadbent remains vocal in parliament to this day, has congratulated Port Hedland Council for calling for an end to COVID vaccines and has furnished Australia’s PM with material on the matter. Broadbent raised his concerns in parliament on 18 November, and I recommend watching this 5 minute video of him speaking.
Another voice to echo Julian Gillespie, is erstwhile ABC journalist Maryanne Demasi. Perhaps her contribution is best summed up in the COVID vaccine conspiracy film she narrated, The Truth – About COVID-19 shots. Erroneously labeled a documentary, it was raved about by Gillespie. And understandably so, given that it includes all his favourite vaccine conspiracies, champions the case and complaints associated with Fidge v Pfizer and lists Gillespie as a source. Demasi also has a Substack account, and has kept her subscribers up to date with DNA contamination developments. In addition Demasi claims the TGA “hides from” reports of SIDS, post vaccination, the TGA and FDA ignored DNA contamination of the HPV vaccine Gardasil, and of course that the TGA response to the claim that mRNA vaccines exhibit DNA contamination, is wrong.
As The Australian Vaccination-risks Network celebrate thirty years of spreading anti-vaccine and dangerous health advice to unsuspecting Australians, some satisfying memories of yesteryear have come to mind. Foremost is the delightful own goal scored by AVN founder Meryl Dorey, when promoting Black Salve as she bemoaned the Therapeutic Goods Administration (TGA) for taking action against the AVN for advertising a DVD, which itself promoted Black Salve. Let me explain.
It all began way back in 2012 with increasing interest in a fraudulently marketed so-called skin cancer “cure”. Namely, a corrosive salve known as an escharotic, being marketed as the near-miraculous Black Salve. A DVD sold by the (then) Australian Vaccination Network (AVN) titled One Answer to Cancer, was packed with anecdotal testimonies praising Black Salve and criticising Aldara, the medically approved treatment for keratoses and superficial basal cell carcinomas. I blogged about this at the time, and you can catch up here. It’s indicative of how quickly interest in Black Salve and the dubious DVD was spreading, to see that on 19 March 2012 the TGA published a warning about black and red salves in treating cancer. This included:
The recent use of products marketed as containing ‘Black salve’ in Australia has resulted in serious harm to the skin of three Australian consumers who used the black salves for various skin conditions including the treatment of a skin cancer.
The TGA is not aware of any credible, scientific evidence which shows that any black or red salve preparation is effective in treating cancer. These types of salves have not been formally assessed by the TGA and are not included in the Australian Register of Therapeutic Goods or exempted from inclusion.
All therapeutic goods, including those used for treating cancer, must be included in the Register unless exempted. Penalties of up to $5.5m apply to the illegal importation or supply of therapeutic goods.
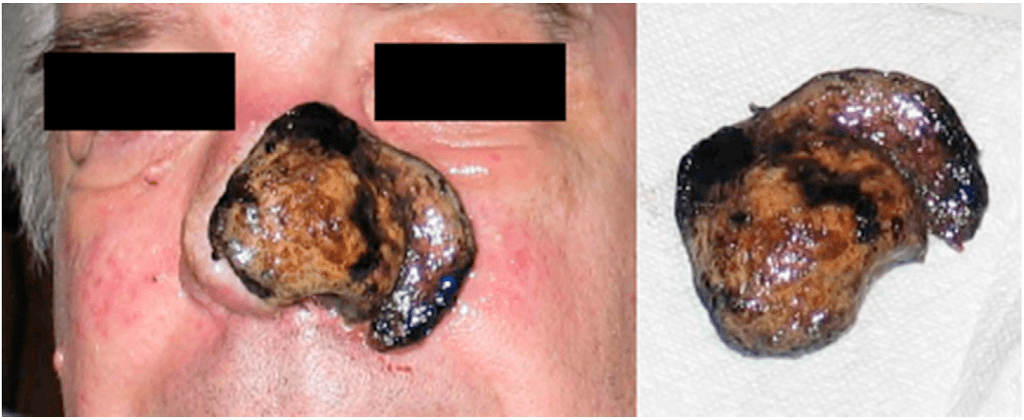
The TGA was investigating importation and a complaint made about supply via the internet. The Australian Pesticides and Veterinary Medicines Authority were also investigating sales purportedly proffered for pets. The TGA stressed that the problem with corrosive salves is that they “essentially burn off layers of the skin and surrounding normal tissue. They can destroy large parts of the skin and underlying tissue, and leave significant scarring.” The corrosive quality is unpredictable and almost impossible to control. Indeed Black Salve is also referred to as a pro-necrotic agent, which I blogged about in 2019. Once the process begins, widespread necrosis follows, leading to the release of enzymes which cause the breakdown of neighbouring cell membranes. A domino effect ensues causing widespread cell death. It brings to mind the “acid for blood” scene in the movie, Alien.
Necrosis of left nostril and surrounding tissue caused by Black Salve (Wikipedia)
Proponents misleadingly call it Nature’s Scalpel. The purpose of One Answer to Cancer was to promote Black Salve and offer instructions on how to prepare your own batch, using zinc chloride and sanguinaria canadensis, also known as bloodroot. This way the DVD producers could side step charges of selling the illegal corrosive. In December 2018, The Royal Australian College of General Practitioners published a comprehensive article on Black Salve, its history and use, noting that the main ingredient is the synthetic corrosive, zinc chloride. Thus claims of a “natural alternative” are inaccurate, and “catastrophic consequences can occur”. The dangers were well documented in 2012 and warnings were abundant. Nonetheless, in the AVN shop Meryl Dorey had included the following blurb with the DVD ad’.
50% of us will face cancer in our own lives at one time or another… we will have to face the choice of how to treat our illness – using toxic drugs or safe, effective, time-tested natural remedies… If you or someone you know is facing this issue or if you just want to be prepared for any future cancer diagnoses, this will be the best $25 you have ever spent!
The advertisement was in breach of the Therapeutic Goods Act 1989 (the Act) and numerous sections of the TGA Advertising Code (the Code). The Code is an effective legislative device for drawing up complaints against the peddling of quack remedies. Once content meets the definition of an advertisement, that content is subject to a number of principles outlined in the Code. More so, persons who publish what meets the definition of an advertisement may be guilty of an offence if other other medications are criticised or if a risk of harm applies. To read the advertisement and understand how the Code and the Act applied in 2012 you can check out the complaint I lodged on 19 April that year.
Prior to 1 July 2018, advertising complaints lodged with the TGA were handled by a Complaints Resolution Panel (CRP). A media release announcing that the TGA would take on the role of complaint management is available here. Way back in 2012 my complaint was handled by the CRP, and their findings from December 2012, can be accessed here. Fifteen sections of the Code and one section of the Act were found to have been breached. The AVN were told to remove the advertisement and publish the notice below.
However long before this, the TGA informed Meryl Dorey that a complaint had been lodged, as is her right. Unsurprisingly, Meryl felt both the complaint and the request of the TGA to remove the offending advertisement was an abuse of her network’s rights. On 5 May 2012, which was about two weeks after being notified, Meryl gave an interview on Fairdinkum Radio, a production of Resistance Media. This was an early freedom fighter production, and host Leon Pittard opened the show announcing the title as, The Australian Government’s Assault on Health Freedom. For me, the highlight of the show was Meryl’s interview which you can access below, or download here.
Meryl waxed lyrical about the benefits of Black Salve and the horror of Aldara, which she falsely claimed was “banned in many parts of the world”. Meryl also managed to call the TGA Cost Recovery model, “a fairly evil policy”. She provided a dubious anecdote of her own apparent use of Black Salve and wrongly claimed it has a “two thousand year history”. She mentioned the DVD and wrongly claimed Black Salve was a combination of herbs and minerals. The interview went on for over five minutes and easily met the definition of an advertisement. An advertisement for Black Salve published in broadcast media, no less. I lodged a second complaint.
The complaint makes clear how both Meryl and host Leon Pittard were liable as advertisers. It also contains a transcript of the interview. Application of appropriate sections of the Code, the Act and the Therapeutic Goods Regulations 1990, justified removal of the interview/advertisement and publication of a retraction (below). By the end of January 2013 the CRP had published their findings which can be accessed here. Thirteen sections of the Code were breached along with two sections of the Act. No sections of the Code raised in the complaint were found not to be breached. More so, over five paragraphs the panel raised additional matters not in the complaint. These included a possible breach of the Act relating to the Register of Therapeutic Goods, and nine possible breaches of the Code relating to criticism of Aldara, promoting a dangerous compound for serious disease, comments about the TGA and more (see pp. 2-3).
Page 3 of the CRP report includes reference to a somewhat bizarre response to a member of the panel from both Dorey and Pittard. In essence they would cop to the findings of the panel if the member would, in his private capacity, present “true, complete and correct proof” that relating a personal condition to anyone constitutes advertising, that the person making the claim is aware of fees paid for advertising, that free speech is not an inherent right, that any corporation has the right to sue an individual and that the matter couldn’t be settled in private. Leon Pittard had long boasted of monitoring the New World Order, employed a watered-down sovereign citizen logic to his world view and, like Dorey, was a fan of conspiracy theorist, Senator Malcolm Roberts. Pittard no doubt penned the response attributed to both he and Dorey (summarised below).
To my surprise, a short time after lodging the complaint I stumbled across this ridiculous video from the USA which was defending the position of Leon Pittard and Meryl Dorey. I wonder if in the rush to defend free speech the producers did any serious research on Black Salve, or understood the danger their support posed to an unsuspecting public.
Ultimately it was rewarding to have these particular complaints upheld. The second complaint – a veritable own goal – was particularly satisfying. However as is often the case with groups beholden to anti-science ideologies and belief in a fight for “health freedom”, such advertisements aren’t always removed when requested. Non-compliance is met with further warning notices, whilst more serious penalties reflect the nature of the breach and risk to the public. There’s little doubt that Black Salve caused serious injuries at the time and a quick search reveals that it continues to cause harm and generate health authority warnings in developed nations. The TGA seized Black Salve capsules on the Gold Coast in May 2019 and again in Brisbane, in December 2023.
The TGA publish regulatory decisions and announcements and the outcomes of advertising compliance investigations. As members of the public it’s up to us to report harmful products and dodgy advertisements to the TGA. It may involve a bit of reading but not every complaint needs to begin with every potential breach.
You can report perceived breaches or questionable practices here. There’s more information on reporting, what you need to provide and accessing support to complete forms here.
On 23 August this year, Robert F. Kennedy Jr. suspended his independent US presidential campaign in ten battleground states, choosing to endorse Donald Trump. He cited the same causes, “that persuaded me to leave the Democratic Party and run as an independent”, according to AP News. Namely, free speech the war in Ukraine and “a war on our children”.
Kennedy: Anti-vaccine activist
There is, of course, no war on American children. Nor a war on any children in developed nations, in the sense Kennedy is alluding to. In fact as the chairman of Children’s Health Defense (CHD), Kennedy has himself waged a long battle against one of public health’s most important pillars; childhood immunisation. As with every anti-vaccine activist, COVID-19 presented Kennedy with an opportunity to manipulate and exploit a growing pool of misguided and misinformed individuals. Those who blame COVID-19 vaccines for virtually every illness or cause of death. Let me stress, I’m not referring to the known side effects but rather, those pushed by COVID conspiracy theorists and tireless anti-vaxxers. Ultimately, Kennedy’s profile expanded markedly, as did CHD revenue.
So comfortable with deceit, when he began his independent trot toward the White House, Kennedy insisted he was not anti-vaccine. This, despite telling a supportive crowd in December 2021, “It is criminal medical malpractice to give a child one of these vaccines”. Despite his influence in bringing about the measles tragedy in Samoa. He worked hard at the presidential pretence, even temporarily stepping down from his position as CHD Chair. Still today, the “chairman on leave” video message on every CHD website page lacks any reference to vaccines. Yet Kennedy mentions “unnecessary injuries” suffered by children, includes studies of autism and developmental disorder rates and packs in 16 snippets of autistic individuals – mostly with pronounced symptoms. Children are chronically sicker than ever before, “wandering around in a toxic soup”, Kennedy tells viewers. In search of the cause he will die with his boots on, fighting for them. Kennedy originally wrongly linked vaccines to autism in a, now removed, 2005 Rolling Stones article. This fact check piece offers an excellent deconstruction of the misconceptions used to make that link.
Vaxxed
Kennedy’s Children’s Health Defense has been hard at work targeting vaccine evidence during the COVID pandemic. This includes the making of the third Vaxxed film, Vaxxed III: Authorised to Kill, by CHD Films. True to the Vaxxed brand, it is a slick cornucopia of fear-mongering and falsehood. A key figure in this ghastly enterprise is interviewer and co-producer Polly Tommey, who has been involved with the first two Vaxxed films. Readers may remember Tommey was banned from Australia for three years following her antics in promoting the original Vaxxed film here in 2017. Trundling about with the (then) Australian Vaccination-skeptics Network, Tommey, who wrongly believes the MMR vaccine caused her son, Billy, to develop autism, told Australian audiences “doctors were murderers”. The Tommey named as producer of Vaxxed III and Vaxxed II: The people’s truth, is her other son, Tobias. The second and third Vaxxed films have been directed by Brian Burrowes. The first Vaxxed was directed by Andrew Wakefield and produced by Del Bigtree.
In doing some basic research for this post, I noted that Polly Tommey has changed not at all. On 6 September she used CHD’s X account to peddle the falsehood that “an experimental” oral polio vaccine is being used in Gaza. She added the sweeping claim that “the oral polio vaccine” is responsible for the poliovirus infecting “hundreds each year”. Like most persistent anti-vaccine lies there is a kernel of truth here. A prior oral polio vaccine caused disease in ~1 in 2.9 million. However, the new oral vaccine in Gaza does not contain the vaccine-derived strain responsible for past infections. More so, it is the lack of vaccination and the presence of poliovirus in human waste causing the problem. In addition, removal of the problematic weakened virus in 2016, in an attempt to prevent vaccine-derived outbreaks, resulted in greater infection rates. Citing a draft report for the World Health Organisation, AP News explain:
The polio strain in question evolved from a weakened virus that was originally part of an oral vaccine credited with preventing millions of children worldwide from being paralyzed. But that virus was removed from the vaccine in 2016 in hopes of preventing vaccine-derived outbreaks.
Public health authorities knew that decision would leave people unprotected against that particular strain, but they thought they had a plan to ward off and quickly contain any outbreaks. Instead, the move resulted in a surge of thousands of cases.
Suffice it to say, facts are anathema to CHD and Tommey. Which brings us to the quality of Vaxxed III: Authorised to Kill. As with the prior two films the main content is of people interviewed about so-called “vaccine injuries”, deaths and negative health system experiences, filmed in a Vaxxed bus driving across the USA. Like all Vaxxed buses this one was wrapped in Vaxxed brand colour and font. This time the message was Vax – UnVax: The People’s Study. The journey took nine months. All the COVID-19 anti-vaccine tropes are there. Countless testimonies of “life-altering injuries and deaths”, frightening symptoms, scans of brain tumours and pulmonary bleeds, suicidal tendencies and futile hospitalisations. Whistleblowers, medical professionals and lawyers apparently serve to legitimise what is unmitigated disinformation. Viewers are primed to accept that any response to COVID was a “fundamental violation of human rights”.
Vaxxed films are slick productions. Well edited to give the impression of government and health-authority deception, feeding viewers a misleading narrative that casts vaccines as harmful toxins pushed onto an unsuspecting public for nefarious reasons. A conspiracy to hide the truth is always present. As with all Vaxxed buses the names of the “vaccine injured” and dead are written on the outside of the bus. The dedication page for these most recent names contains over 1,350 entries, many of which list autism from MMR or “childhood vaccinations”. Apart from harm done to perception of vaccine safety and public health, individuals exploited and coaxed into a victim mindset, experience genuine pain and distress. Nothing good comes from these films.
Message on the CHD Vaxxed bus
This latest Vaxxed chapter raises a few questions for those of us in Australia who followed the antics of The Australian Vaccination-risks Network (AVN) and their much troubled journeys in their own Vaxxed II: The People’s Truth, bus. The AVN hit the road in July 2020 in their bus, sticking closely to the Vaxxed script. They clocked up seven seperate tours in two buses, as the first was irreversibly damaged in NSW flood waters. On 8 July 2020, AVN founder Meryl Dorey revealed parents “will be filmed for an up-coming Australian documentary”. Five weeks earlier president Anita Hafemeister had boldly claimed, “This will be the Australian version of Vaxxed II, I assume”. All that excitement led this humble author to speculate that the Vaxxed II bus tour would yield material for Vaxxed III. In fact the AVN was still advertising the bus, with sponsorship requests, in February this year. One can only assume that the reality of CHD dollars, Kennedy’s backing and the ambition of Polly Tommey has for now, kept content from Down Under off the big screen.
Polly Tommey and CHD are pushing to fill theatres in the US for an 18 September screening. A host of graphics are offered to assist fans to spread the word on social media. All contain the image of a driverless bus emerging from the mist in the dead of night. The film is being advertised with an unabashed call for donations. Or if you’d like to be an associate, co-‘ or executive producer with a minimum donation of $10,000, that privilege is a mere phone call away. No doubt Vaxxed III will make a profit for Kennedy’s CHD.
Of more concern, is that acceptance of COVID vaccine misinformation has grown in developed nations under the labour of anti-vaccine activists. The USA is currently experiencing a growth in the belief of COVID vaccine falsehoods and this film, along with the discussion that follows, may well worsen that trend in the US and elsewhere. Australian anti-vaxxers will have to wait for an online release.
Polly Tommey and Co discuss pre-release debunking of Vaxxed III
Last week Jane Hansen passed away from glioblastoma, an aggressive form of brain cancer. Jane was a deeply committed and focused journalist who utilised evidence to challenge pseudoscience, scams and disinformation. Jane regularly used truth to expose those who profited from exploitation of the vulnerable. She had journalistic skills equal to multiple tasks. Her presentation style and writing made that abundantly clear.
Consequently, Jane’s colleagues have recently offered other adjectives to describe her as a journalist. Esteemed, celebrated, legendary, star, courageous, compassionate, revered, renowned, tireless, passionate, crusader, genuinely funny, a giant, a hero, a pioneering female, a warrior for truth. Social media reflected the extent of the respect Jane had engendered over the years. Amazing, awesome, tireless warrior, dedicated, excellent, great… and more. A quick search for Jane’s name yields a veritable stampede of honorific headlines, all jostling to make individual statements, yet all condensing around one notion: Praise.
Respected Australian journalist, Ray Martin offered this summary:
“Jane Hansen gave journalism a good name. She was formidable, energetic and ethical.
“She fought relentlessly for the underdog and the disadvantaged – especially women and Indigenous Australians.
“Jane was smart, funny and a reliable friend. We’ll miss her pursuit of excellence, as she tried to keep the bastards honest.”
Jane was also a loving and loved mother, sister and an adored friend of many. I knew Jane only through the occasional email exchange or direct messaging on social media, yet often enjoyed her well known talent for making people laugh. I’ve lost count of the number of times I consulted an article Jane had written to orient myself regarding a specific anti-vaccine insult, or from whom a certain deceit had arisen. One highlight for me was Jane’s work in the making, production and promotion of Big Shots: Anti-Vaxxers Exposed. Made in the early, pre-vaccine days of the COVID-19 pandemic, Jane capably bridged the harm that anti-vaccine lobbying had already caused in Australia, and the foreseeable damage COVID conspiracy theories would inevitably bring.
Readers familiar with the tactics of vaccine conspiracy theorists can certainly guess, or may well be aware, of how they have reacted to this news. Fortunately, Jane made a lasting schism in their fragile credibility, leaving in her wake a surging wash of evidence-based reasoning, powerful enough to smother both their deceit and vulgarity. Jane always focused on presenting the facts. Her critics focused on attacking the person. On the day Big Shots aired in 2021, Jane was interviewed on Sky News, and shared this observation, which in my mind reflects both her sense of fairness and respect for sound public health.
I don’t have a problem with questioning a vaccine. This is a new vaccine, we want to know if it’s safe. There’s no point in having an unsafe vaccine; we all want a safe vaccine. But some of the misinformation that’s being spread is just ludicrous.
Jane’s career was extensive, including her role as a war correspondent for Network 10 in both Iraq and Bosnia, later working on the current affairs programme Hard Copy. She worked at Channel Nine for fourteen years. Jane co-authored Boned, the eye-opening book on boys-club mentality in TV media, and also authored the deeply personal and emotional Three Seasons. Her own experiences aided her unbiased assessment of Kathleen Folbigg, culminating in Jane writing and presenting the popular podcast Mother’s Guilt. Of course, Jane also managed her extensive and impressive career at The Sunday Telegraph.
Jane’s tireless campaigning was instrumental to the introduction of the Abbott/Turnbull government’s No Jab, No Pay/Play policies. Introduced in 2016, this public health initiative has seen an ongoing increase in life-saving childhood vaccination and is regarded as an overwhelming success. Jane’s reporting on anti-vaccine responses to it continue to educate the community. The same can be said for her criticism of anti-fluoridation conspiracies. In 2018 Jane was the inaugural winner of The Barry Williams Award for Skeptical Journalism. Australian Skeptics Inc. explain:
The Barry Williams Award for Skeptical Journalism is awarded for journalistic work that critically analyses or exposes issues related to pseudoscience or the paranormal. The award is dubbed “The Wallaby” after Barry’s alter ego of Sir Jim R Wallaby, which he used for some of his more whimsical pieces published in The Skeptic magazine. In addition to a commemorative certificate, $2000 is awarded to the recipient or to a charity or cause of their choice.
Jane Hansen awarded the “Wallaby” 2018
Jane’s respect for evidence-based public health policies was linked to her desire for a more just world. In addition to her work exposing pseudoscience, Jane also reported on childhood muscular dystrophy, childhood medication, childhood cancer, cardiac health, teen vaping, IVF clinics, endangered animals, diabetes, organ donation and much more. Claire Harvey described Jane as “the most passionate journalistic crusader” she’d ever known. Jane’s work will remain and continue to positively influence others.
As a final note I’d like to stress there is no such thing as turbo cancer and no evidence COVID-19 vaccines cause cancer. Jane passed away late on 6th August after being diagnosed less than two years ago with glioblastoma, a particularly aggressive form of brain cancer. Outside of inherited syndromes or exposure to radiation, the cause of glioblastomas is not known. More common in older adults, they may occur at any age. Research has not identified anything that can prevent development of glioblastoma.
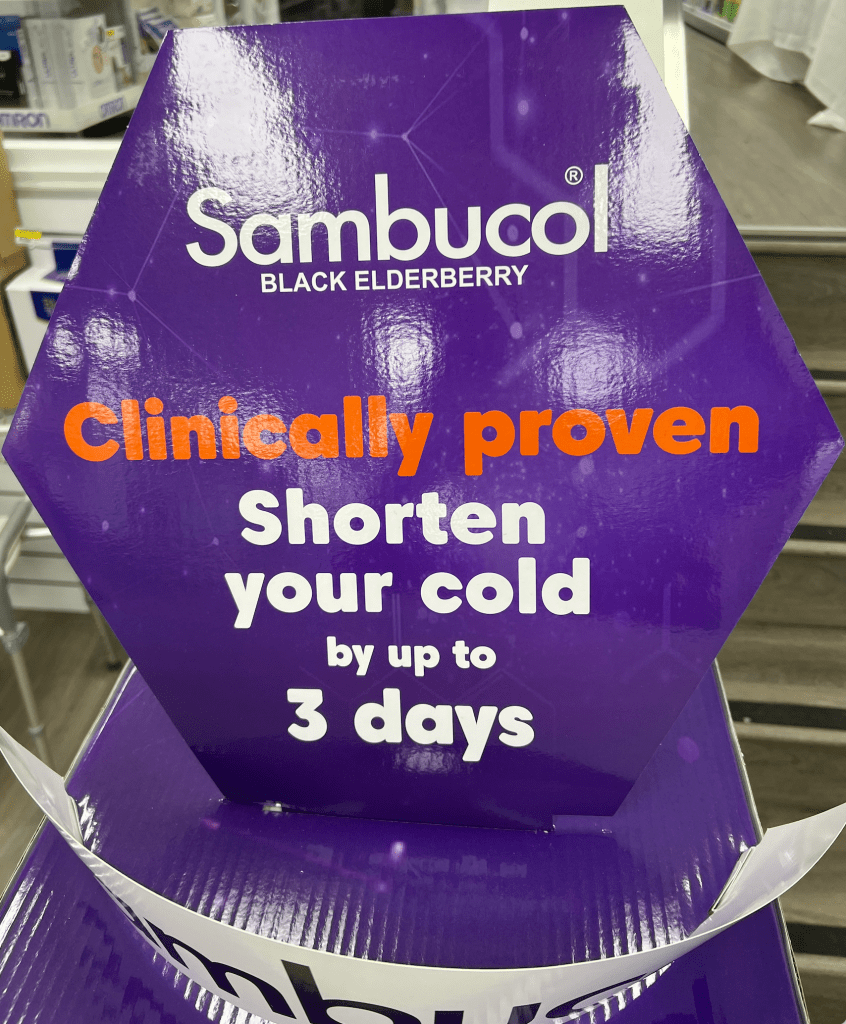
A couple of weeks before the start of winter, I wandered past a garish product display in my local pharmacy. A glossy purple hexagon boasted orange font across its middle; Clinically proven. Underneath that in white font: Shorten your cold by up to 3 days.
Taking in the entire sign, I spotted a familiar brand name. Sambucol® – Black Elderberry, a product of PharmaCare. The hexagon sat atop five cardboard shelves each labelled with more claims: Feel Better Faster, Intensive Immune, Shorten Your Cold, all packed with something for “kids”. Immune Defence Gummies,Soothing Throat Pops and Soothing Lozenges to “refresh the nose and throat”. It all sounded wonderful. I mean, who doesn’t want to feel better faster? Or puff up immunity with gummies? And knock 3 days off a cold? Surely it wasn’t just for kids. Then I wondered, could such claims really be “clinically proven”?
The elderberry grows on the elder plant (Sambucus nigra). Nataly Martini of the School of Pharmacy at the University of Auckland has written about elderberry in the Journal of Primary Healthcare, 31 March 2021 (2021;13(1):91–92. doi:10.1071/HC15960). It is reproduced by the Royal NZ College of General Practitioners, as a Potion or Poison article accessible here. The author notes “Dried or fresh berries have been used to treat constipation, neuropathic pain, headache, tooth-ache, sinus congestion, sore throat, influenza and the common cold, among others”. A meta-analysis of four randomised placebo-controlled studies, often cited by Pharmacare in promoting Sambucol, is also referenced. Martini reports that supplementation with elderberry, “reduced the duration of upper respiratory symptoms in verified cases of influenza, or symptoms consistent with either influenza or the common cold, when administered at the onset of symptoms”.
Martini continues:
Other studies have reported that elderberry supplementation significantly reduced symptoms and the duration of influenza A by 3–4 days, or the common cold by ~2 days in long-haul travellers. However, in the latter study half of the participants also used co-medication to relieve symptoms, limiting the application of these findings.
Writing in The Conversation Monash immunology researcher Kim Murphy referred to the latter study noting the collective duration of colds, rather than the average length, was compared in unequal group sizes, and concluded, “this isn’t a reliable finding”. What stands out in Martini’s article is the Summary Message. It highlights a recurring theme with the efficacy of elderberry preparations and symptom duration. Namely, that more research is needed to substantiate claims and high quality trials are currently lacking:
Although findings suggest that elderberry may be effective in reducing symptoms and duration of viral infections, more high-quality human trials are needed to substantiate these claims. Currently no studies support the use of elderberry in coronaviruses. Generally regarded as safe, toxicity may result from ingestion of raw or uncooked fruit, and allergies may occur in susceptible people. Use is not recommended in pregnancy and lactation due to insufficient evidence. Elderberry products may exacerbate symptoms in patients with autoimmune diseases. Caution is advised with immunosuppressants as elderberry may reduce effectiveness of these drugs. No major drug interactions are known.
Pharmacare is an alternative medicine manufacturer, and as such its primary concern is brand promotion and brand protection. In essence, Pharmacare is about sales. There’s nothing wrong with this, but as a skeptic I’m more concerned with the transparency of the claim that Sambucol® is “clinically proven” to reduce cold symptoms by up to three days. Can such a claim be trusted? Let’s review a 2018 article by Liam Mannix, science reporter for The Age and Sydney Morning Herald; University of Sydney pulls claims elderberries can fight flu, to get our bearings. The article opens:
One of the country’s leading universities has been forced to retract a claim its study showed eating elderberries could help beat the flu after admitting it was overhyping its own science.
The University of Sydney also concealed the research was part-funded by company Pharmacare – which sells elderberry-based flu remedies – at the company’s request. Although it was declared in the study itself, the university also failed to publicise that a Pharmacare employee was involved in the research.
The flu-busting claim, made in a press release and published on the university’s website, attracted national and international media attention, most of which did not mention the Pharmacare funding.
The article reveals that the study simply focused on in-vitro dosing of human cells in a laboratory environment. No mice or human subjects were involved. As stressed in the article such research is fine, but how it is represented is vital. Professor Ken Harvey, then-president of Friends of Science in Medicine observed:
“This is an appalling misrepresentation of this Pharmacare-funded in-vitro study. It was inappropriate and misleading to imply from this study that an extract was ‘proven to fight flu’.”
The article reveals that Pharmacare were aware of the press release but requested not to be named, for reasons study authors did not understand. Ray Moynihan, an assistant professor at Bond University’s Centre for Research in Evidence-Based Practice, who studies science reporting in the media stressed it raised “serious concerns” about transparency. “It is vital information for us to know who sponsored the study“, he said at the time.
The Sydney Uni episode said much about Pharmacare transparency and even more about claims relying on Pharmacare-funded studies. The company presently has a collection of articles gathered to back its many assertions. Some cite Pharmacare studies, whilst others present generalised health-related information, citing other studies, articles and reports. Following Sambucol® “shortening colds by up to 3 days” brings us to a page that opens with:
Sambucol® Black Elderberry Cold & Flu is the only Black Elderberry Cold & Flu product clinically proven to shorten your cold by up to 3 days.
The page refers to a study by Rao A, et al, and informs the reader it is an, “Unpublished study by RDC Global on behalf of Pharmacare Laboratories. Available on request.” More about this study, can be gleaned from a Pharmacare internal catalogue on their Clinically Proven Formula, which is marked on each page, “For Professional and Internals Staff use only. Not to be distributed”. The catalogue includes a number of Pharmacare-funded studies, and lists the Rao et al, study title in full: Rao A, Sethi M, Dick C, A double-blind, randomized, placebo-controlled study to evaluate the safety and efficacy Sambucol® liquid formulation to reduce the duration and severity of the common cold symptoms in adults. PHA-Sam15. 2016.
The catalogue summary of the study, offers graphs and a report on p.6. It professes a 31.8% reduction in symptom severity and a reduction in sick days from 8.9 to 5.9 (33.7%) days between placebo and Sambucol® recipients. The public summary includes:
The efficacy of Sambucol Black Elderberry Cold & Flu to reduce the duration and severity of common cold symptoms was researched in a double-blind, randomised and placebo-controlled study sponsored by Pharmacare Laboratories.
The study included 461 healthy, adult participants and found that participants who took Sambucol® Black Elderberry Cold & Flu daily from the onset of cold symptoms were sick for a significantly shorter period of time.
The median duration of illness for the placebo group was eight days, whereas the median duration of illness for the group taking Sambucol® Black Elderberry Cold & Flu was five days – a median three-day reduction in duration of illness.
According to the study, “The results show that supplementation with Sambucol® Black Elderberry Cold & Flu at the onset of cold symptoms significantly reduced the duration of a cold episode as well as significantly reduced the severity and impact of cold and flu symptoms.
Being unpublished, the Rao et al, study lacks the authority attributed to peer reviewed research. Nor has it been reproduced independently. Yet Pharmacare-funded studies are of paramount importance to their business model. It allows the company to produce and distribute positive material related to Pharmacare brands. As the FAQ page informs us under, What is the difference between Sambucol Black Elderberry products and other black elderberry products?
Not all black elderberry extracts are the same. Only Sambucol Black Elderberry, the original black elderberry extract introduced more than 20 years ago, contains the same proprietary, naturally balanced elderberry extract used in the published scientific studies. Other products use a concentrated, standardized elderberry extract. They are fundamentally different ingredients.
Pharmacare Brands
Nonetheless, the internal Pharmacare catalogue cites a number of studies where generic elderberry extract is used, to assert its effect on the duration and impact of cold and flu symptoms. There have been no comparative studies of extract efficacy, and as such there is no evidence that Sambucol® Black Elderberry is more or less effective than any other black elderberry extract. Generic extracts have been used in “the published scientific studies”, such as the Hawkins et al meta-analysis, which found an association with reduced influenza A symptoms and duration.
Speaking of influenza, Pharmacare cite two studies in their internal catalogue that conclude Sambucol® has an effect against influenza. On page 6 they refer to in-vitro and in-vivo efficacy against influenza A and B. On page 7 they refer to in-vitro efficacy in reducing H5N1 by 99%. The catch for Pharmacare here, is that Australia’s Therapeutic Goods Administration (TGA) limit the seriousness of diseases and symptoms that they can claim Sambucol® relieves. Influenza is not accepted (see below). On another note, one must be aware that Pharmacare’s Sambucol® benefits from generic use of the term Sambucol. Consider this entry for Sambucol at drugs.com.
Sambucol is a berry from a European or Black elder tree. The berries are used to make medicine. Sambucol is also known as Arbre de Judas, Baccae, Baises de Sureau, Black-Berried Alder, Black Elder, Boor Tree, Bountry, Elderberries, Ellanwood, Ellhorn, European Alder, Fruit de Sureau, Grand Sureau, Hautbois, Holunderbeeren, Sabugeuiro-negro, Sambequier, Sambu, Sambuc, Sambuci Sambucus, Sambugo, Sauco, Saúco Europeo, Schwarzer Holunder, Seuillet, Seuillon, Sureau, Sureau Noir, Sus, Suseau, or Sussier.
The emerging claim that Sambucol® improves immunity also deserves comment. The internal catalogue summarises a 2002 study by Barak et al, on page 8, with the conclusion:
Sambucol® activate the healthy immune system by increasing inflammatory cytokine production more effectively compared to other herbal remedies.
The study, The effect of herbal remedies on the production of human inflammatory and anti-inflammatory cytokines compared Sambucol® to propolis and Echinacea. These are used as herbal treatments and preventatives of upper respiratory tract infections in adults and children. The cytokine-modulating effect of echinacea has been demonstrated in-vitro and in animal studies. However, a 2021 systemic review concludes firm evidence linking elderberry to inflammatory cytokine production is lacking. However, accounts of elderberry syrup linked to Drug Induced Liver Injury and Autoimmune Hepatitis have become evident. In the latter case the overproduction of inflammatory cytokines has been considered. Depending on future incidence, proper management at the point of sale may thus require an understanding of patient history. Whilst this is possible in the pharmacy setting it is not so elsewhere.
The claimed reliability of elderberry lends itself to the appeal to antiquity as it has reportedly been used for centuries, for a host of purported reasons, as mentioned above, in addition to heart disease, gum disease, high cholesterol and obesity. The drugs.com entry for Elderberry and Sambucol are identical and include (bold mine):
It is not certain whether [Sambucol/Elderberry] is effective in treating any medical condition. Medicinal use of this product has not been approved by the FDA. This medicine should not be used in place of medication prescribed for you by your doctor.
The US Food and Drug Administration (FDA) have warned promoters of elderberry syrup, as evidenced by (for example) a September 2000 warning letter and another in August 2022, written to highlight breaches of the Federal Food, Drug and Cosmetic Act because the products advertised were “intended for use in the cure, mitigation, treatment, or prevention of disease”. The FDA does not regulate herbal supplements. In Australia the TGA accepts Sambucol Black Elderberry Cold & Flu and Sambucol Black Elderberry Cold & Flu + Pain as Listed medicines as opposed to Registered medicines.
Read more about TGA classifications here, and please remember a September 2022 TGA review of Sambucol® states, “The efficacy of the medicine was not assessed as part of this review”. Thus the term “TGA Assessed” cannot be used in relation to this product or on its label. Read more about TGA regulation of Listed medicines here. The TGA does not approve Listed medicine labels before marketing. The TGA state:
This is because we take a risk-based approach to regulation, which means higher risk medicines have more rigorous controls than lower risk medicines. However, we do require sponsors to certify that the medicine complies with all relevant regulation, and that they hold evidence that their medicine does what it says it will. Source: TGA – How we regulate medicines.
The public summary on the TGA Australian Register of Therapeutic Goods for Sambucol Black Elderberry Cold & Flu permits the following indications.
Relieve weariness/tiredness/fatigue/feeling of weakness.
Maintain/support general health and wellbeing.
Decrease/reduce/relieve common cold duration.
Helps decrease/reduce/relieve the severity of symptoms of common colds and flu.
Decrease/reduce/relieve symptoms of common colds and flu.
Label statement: If symptoms persist, talk to your health professional.
Product presentation must not imply or refer to serious forms of respiratory disorders/diseases, such as: asthma, pneumonia, COAD, COPD, influenza.
Label statement: Adults only, OR Not to be used in children under 2 years of age without medical advice (or words to that effect).
Respiratory tract infections must be qualified by ‘mild’.
Product presentation must not imply or refer to chronic fatigue syndrome.
Looking at the above it is clear the TGA have been more than generous with the allowed claims in the ARTG indications for this product. Particularly given the lack of published evidence and the absence of TGA assessment for efficacy. I don’t accept that Sambucol is clinically proven to shorten colds or boost immunity or any other claims made in sales promotion. The evidence simply isn’t there and relying on unpublished work organised and funded by Pharmacare is misleading. Whilst an impact of elderberry syrup on cold and flu symptoms is acknowledged in literature, the most common conclusion is that more research is needed. Quality human trials are still lacking.
So what might Pharmacare have planned to improve evidence in their favour? The Australian New Zealand Clinical Trials Registry, presently has the registered trial ACTRN12623000299606, last updated 7 April 2024. The title is, Determining the effectiveness of Sambucol in reducing the duration and symptoms of the common cold in children and teens. The age group is 2-17 and the aim is to use Sambucol and report on symptoms via, “a purpose-built study app ‘Sambucol Research’.” The methodology is likely to favour Pharmacare, particularly given that there is no control group. Rather, “a comparison will be made to two existing data sets”.
The first data set is reported as:
Data describing the incidence, severity and duration of different cold symptoms in children over a six-week period. (Troullos E, Baird L, Jayawardena S. Common Cold Symptoms in Children: Results of an Internet-Based Surveillance Program. J Med Internet Res. 2014 Jun 19;16(6):e144.) This study was not a randomised controlled trial or an intervention. The study observed duration and severity of colds and as such was not registered.
The second data set is “a confidential report to Pharmacare”, and is none other than the initial unpublished study that found Sambucol® “shortened colds by up to 3 days”; Rao A, Sethi M, Dick C. A double-blind, randomised, placebo-controlled study to evaluate the safety and efficacy of Sambucol liquid formulation to reduce the duration and severity of the common cold and flu symptoms in adults.