Last week Jane Hansen passed away from glioblastoma, an aggressive form of brain cancer. Jane was a deeply committed and focused journalist who utilised evidence to challenge pseudoscience, scams and disinformation. Jane regularly used truth to expose those who profited from exploitation of the vulnerable. She had journalistic skills equal to multiple tasks. Her presentation style and writing made that abundantly clear.
Consequently, Jane’s colleagues have recently offered other adjectives to describe her as a journalist. Esteemed, celebrated, legendary, star, courageous, compassionate, revered, renowned, tireless, passionate, crusader, genuinely funny, a giant, a hero, a pioneering female, a warrior for truth. Social media reflected the extent of the respect Jane had engendered over the years. Amazing, awesome, tireless warrior, dedicated, excellent, great… and more. A quick search for Jane’s name yields a veritable stampede of honorific headlines, all jostling to make individual statements, yet all condensing around one notion: Praise.
Respected Australian journalist, Ray Martin offered this summary:
“Jane Hansen gave journalism a good name. She was formidable, energetic and ethical.
“She fought relentlessly for the underdog and the disadvantaged – especially women and Indigenous Australians.
“Jane was smart, funny and a reliable friend. We’ll miss her pursuit of excellence, as she tried to keep the bastards honest.”
Jane was also a loving and loved mother, sister and an adored friend of many. I knew Jane only through the occasional email exchange or direct messaging on social media, yet often enjoyed her well known talent for making people laugh. I’ve lost count of the number of times I consulted an article Jane had written to orient myself regarding a specific anti-vaccine insult, or from whom a certain deceit had arisen. One highlight for me was Jane’s work in the making, production and promotion of Big Shots: Anti-Vaxxers Exposed. Made in the early, pre-vaccine days of the COVID-19 pandemic, Jane capably bridged the harm that anti-vaccine lobbying had already caused in Australia, and the foreseeable damage COVID conspiracy theories would inevitably bring.
Readers familiar with the tactics of vaccine conspiracy theorists can certainly guess, or may well be aware, of how they have reacted to this news. Fortunately, Jane made a lasting schism in their fragile credibility, leaving in her wake a surging wash of evidence-based reasoning, powerful enough to smother both their deceit and vulgarity. Jane always focused on presenting the facts. Her critics focused on attacking the person. On the day Big Shots aired in 2021, Jane was interviewed on Sky News, and shared this observation, which in my mind reflects both her sense of fairness and respect for sound public health.
I don’t have a problem with questioning a vaccine. This is a new vaccine, we want to know if it’s safe. There’s no point in having an unsafe vaccine; we all want a safe vaccine. But some of the misinformation that’s being spread is just ludicrous.
Jane’s career was extensive, including her role as a war correspondent for Network 10 in both Iraq and Bosnia, later working on the current affairs programme Hard Copy. She worked at Channel Nine for fourteen years. Jane co-authored Boned, the eye-opening book on boys-club mentality in TV media, and also authored the deeply personal and emotional Three Seasons. Her own experiences aided her unbiased assessment of Kathleen Folbigg, culminating in Jane writing and presenting the popular podcast Mother’s Guilt. Of course, Jane also managed her extensive and impressive career at The Sunday Telegraph.
Jane’s tireless campaigning was instrumental to the introduction of the Abbott/Turnbull government’s No Jab, No Pay/Play policies. Introduced in 2016, this public health initiative has seen an ongoing increase in life-saving childhood vaccination and is regarded as an overwhelming success. Jane’s reporting on anti-vaccine responses to it continue to educate the community. The same can be said for her criticism of anti-fluoridation conspiracies. In 2018 Jane was the inaugural winner of The Barry Williams Award for Skeptical Journalism. Australian Skeptics Inc. explain:
The Barry Williams Award for Skeptical Journalism is awarded for journalistic work that critically analyses or exposes issues related to pseudoscience or the paranormal. The award is dubbed “The Wallaby” after Barry’s alter ego of Sir Jim R Wallaby, which he used for some of his more whimsical pieces published in The Skeptic magazine. In addition to a commemorative certificate, $2000 is awarded to the recipient or to a charity or cause of their choice.
Jane Hansen awarded the “Wallaby” 2018
Jane’s respect for evidence-based public health policies was linked to her desire for a more just world. In addition to her work exposing pseudoscience, Jane also reported on childhood muscular dystrophy, childhood medication, childhood cancer, cardiac health, teen vaping, IVF clinics, endangered animals, diabetes, organ donation and much more. Claire Harvey described Jane as “the most passionate journalistic crusader” she’d ever known. Jane’s work will remain and continue to positively influence others.
As a final note I’d like to stress there is no such thing as turbo cancer and no evidence COVID-19 vaccines cause cancer. Jane passed away late on 6th August after being diagnosed less than two years ago with glioblastoma, a particularly aggressive form of brain cancer. Outside of inherited syndromes or exposure to radiation, the cause of glioblastomas is not known. More common in older adults, they may occur at any age. Research has not identified anything that can prevent development of glioblastoma.
A couple of weeks before the start of winter, I wandered past a garish product display in my local pharmacy. A glossy purple hexagon boasted orange font across its middle; Clinically proven. Underneath that in white font: Shorten your cold by up to 3 days.
Taking in the entire sign, I spotted a familiar brand name. Sambucol® – Black Elderberry, a product of PharmaCare. The hexagon sat atop five cardboard shelves each labelled with more claims: Feel Better Faster, Intensive Immune, Shorten Your Cold, all packed with something for “kids”. Immune Defence Gummies,Soothing Throat Pops and Soothing Lozenges to “refresh the nose and throat”. It all sounded wonderful. I mean, who doesn’t want to feel better faster? Or puff up immunity with gummies? And knock 3 days off a cold? Surely it wasn’t just for kids. Then I wondered, could such claims really be “clinically proven”?
The elderberry grows on the elder plant (Sambucus nigra). Nataly Martini of the School of Pharmacy at the University of Auckland has written about elderberry in the Journal of Primary Healthcare, 31 March 2021 (2021;13(1):91–92. doi:10.1071/HC15960). It is reproduced by the Royal NZ College of General Practitioners, as a Potion or Poison article accessible here. The author notes “Dried or fresh berries have been used to treat constipation, neuropathic pain, headache, tooth-ache, sinus congestion, sore throat, influenza and the common cold, among others”. A meta-analysis of four randomised placebo-controlled studies, often cited by Pharmacare in promoting Sambucol, is also referenced. Martini reports that supplementation with elderberry, “reduced the duration of upper respiratory symptoms in verified cases of influenza, or symptoms consistent with either influenza or the common cold, when administered at the onset of symptoms”.
Martini continues:
Other studies have reported that elderberry supplementation significantly reduced symptoms and the duration of influenza A by 3–4 days, or the common cold by ~2 days in long-haul travellers. However, in the latter study half of the participants also used co-medication to relieve symptoms, limiting the application of these findings.
Writing in The Conversation Monash immunology researcher Kim Murphy referred to the latter study noting the collective duration of colds, rather than the average length, was compared in unequal group sizes, and concluded, “this isn’t a reliable finding”. What stands out in Martini’s article is the Summary Message. It highlights a recurring theme with the efficacy of elderberry preparations and symptom duration. Namely, that more research is needed to substantiate claims and high quality trials are currently lacking:
Although findings suggest that elderberry may be effective in reducing symptoms and duration of viral infections, more high-quality human trials are needed to substantiate these claims. Currently no studies support the use of elderberry in coronaviruses. Generally regarded as safe, toxicity may result from ingestion of raw or uncooked fruit, and allergies may occur in susceptible people. Use is not recommended in pregnancy and lactation due to insufficient evidence. Elderberry products may exacerbate symptoms in patients with autoimmune diseases. Caution is advised with immunosuppressants as elderberry may reduce effectiveness of these drugs. No major drug interactions are known.
Pharmacare is an alternative medicine manufacturer, and as such its primary concern is brand promotion and brand protection. In essence, Pharmacare is about sales. There’s nothing wrong with this, but as a skeptic I’m more concerned with the transparency of the claim that Sambucol® is “clinically proven” to reduce cold symptoms by up to three days. Can such a claim be trusted? Let’s review a 2018 article by Liam Mannix, science reporter for The Age and Sydney Morning Herald; University of Sydney pulls claims elderberries can fight flu, to get our bearings. The article opens:
One of the country’s leading universities has been forced to retract a claim its study showed eating elderberries could help beat the flu after admitting it was overhyping its own science.
The University of Sydney also concealed the research was part-funded by company Pharmacare – which sells elderberry-based flu remedies – at the company’s request. Although it was declared in the study itself, the university also failed to publicise that a Pharmacare employee was involved in the research.
The flu-busting claim, made in a press release and published on the university’s website, attracted national and international media attention, most of which did not mention the Pharmacare funding.
The article reveals that the study simply focused on in-vitro dosing of human cells in a laboratory environment. No mice or human subjects were involved. As stressed in the article such research is fine, but how it is represented is vital. Professor Ken Harvey, then-president of Friends of Science in Medicine observed:
“This is an appalling misrepresentation of this Pharmacare-funded in-vitro study. It was inappropriate and misleading to imply from this study that an extract was ‘proven to fight flu’.”
The article reveals that Pharmacare were aware of the press release but requested not to be named, for reasons study authors did not understand. Ray Moynihan, an assistant professor at Bond University’s Centre for Research in Evidence-Based Practice, who studies science reporting in the media stressed it raised “serious concerns” about transparency. “It is vital information for us to know who sponsored the study“, he said at the time.
The Sydney Uni episode said much about Pharmacare transparency and even more about claims relying on Pharmacare-funded studies. The company presently has a collection of articles gathered to back its many assertions. Some cite Pharmacare studies, whilst others present generalised health-related information, citing other studies, articles and reports. Following Sambucol® “shortening colds by up to 3 days” brings us to a page that opens with:
Sambucol® Black Elderberry Cold & Flu is the only Black Elderberry Cold & Flu product clinically proven to shorten your cold by up to 3 days.
The page refers to a study by Rao A, et al, and informs the reader it is an, “Unpublished study by RDC Global on behalf of Pharmacare Laboratories. Available on request.” More about this study, can be gleaned from a Pharmacare internal catalogue on their Clinically Proven Formula, which is marked on each page, “For Professional and Internals Staff use only. Not to be distributed”. The catalogue includes a number of Pharmacare-funded studies, and lists the Rao et al, study title in full: Rao A, Sethi M, Dick C, A double-blind, randomized, placebo-controlled study to evaluate the safety and efficacy Sambucol® liquid formulation to reduce the duration and severity of the common cold symptoms in adults. PHA-Sam15. 2016.
The catalogue summary of the study, offers graphs and a report on p.6. It professes a 31.8% reduction in symptom severity and a reduction in sick days from 8.9 to 5.9 (33.7%) days between placebo and Sambucol® recipients. The public summary includes:
The efficacy of Sambucol Black Elderberry Cold & Flu to reduce the duration and severity of common cold symptoms was researched in a double-blind, randomised and placebo-controlled study sponsored by Pharmacare Laboratories.
The study included 461 healthy, adult participants and found that participants who took Sambucol® Black Elderberry Cold & Flu daily from the onset of cold symptoms were sick for a significantly shorter period of time.
The median duration of illness for the placebo group was eight days, whereas the median duration of illness for the group taking Sambucol® Black Elderberry Cold & Flu was five days – a median three-day reduction in duration of illness.
According to the study, “The results show that supplementation with Sambucol® Black Elderberry Cold & Flu at the onset of cold symptoms significantly reduced the duration of a cold episode as well as significantly reduced the severity and impact of cold and flu symptoms.
Being unpublished, the Rao et al, study lacks the authority attributed to peer reviewed research. Nor has it been reproduced independently. Yet Pharmacare-funded studies are of paramount importance to their business model. It allows the company to produce and distribute positive material related to Pharmacare brands. As the FAQ page informs us under, What is the difference between Sambucol Black Elderberry products and other black elderberry products?
Not all black elderberry extracts are the same. Only Sambucol Black Elderberry, the original black elderberry extract introduced more than 20 years ago, contains the same proprietary, naturally balanced elderberry extract used in the published scientific studies. Other products use a concentrated, standardized elderberry extract. They are fundamentally different ingredients.
Pharmacare Brands
Nonetheless, the internal Pharmacare catalogue cites a number of studies where generic elderberry extract is used, to assert its effect on the duration and impact of cold and flu symptoms. There have been no comparative studies of extract efficacy, and as such there is no evidence that Sambucol® Black Elderberry is more or less effective than any other black elderberry extract. Generic extracts have been used in “the published scientific studies”, such as the Hawkins et al meta-analysis, which found an association with reduced influenza A symptoms and duration.
Speaking of influenza, Pharmacare cite two studies in their internal catalogue that conclude Sambucol® has an effect against influenza. On page 6 they refer to in-vitro and in-vivo efficacy against influenza A and B. On page 7 they refer to in-vitro efficacy in reducing H5N1 by 99%. The catch for Pharmacare here, is that Australia’s Therapeutic Goods Administration (TGA) limit the seriousness of diseases and symptoms that they can claim Sambucol® relieves. Influenza is not accepted (see below). On another note, one must be aware that Pharmacare’s Sambucol® benefits from generic use of the term Sambucol. Consider this entry for Sambucol at drugs.com.
Sambucol is a berry from a European or Black elder tree. The berries are used to make medicine. Sambucol is also known as Arbre de Judas, Baccae, Baises de Sureau, Black-Berried Alder, Black Elder, Boor Tree, Bountry, Elderberries, Ellanwood, Ellhorn, European Alder, Fruit de Sureau, Grand Sureau, Hautbois, Holunderbeeren, Sabugeuiro-negro, Sambequier, Sambu, Sambuc, Sambuci Sambucus, Sambugo, Sauco, Saúco Europeo, Schwarzer Holunder, Seuillet, Seuillon, Sureau, Sureau Noir, Sus, Suseau, or Sussier.
The emerging claim that Sambucol® improves immunity also deserves comment. The internal catalogue summarises a 2002 study by Barak et al, on page 8, with the conclusion:
Sambucol® activate the healthy immune system by increasing inflammatory cytokine production more effectively compared to other herbal remedies.
The study, The effect of herbal remedies on the production of human inflammatory and anti-inflammatory cytokines compared Sambucol® to propolis and Echinacea. These are used as herbal treatments and preventatives of upper respiratory tract infections in adults and children. The cytokine-modulating effect of echinacea has been demonstrated in-vitro and in animal studies. However, a 2021 systemic review concludes firm evidence linking elderberry to inflammatory cytokine production is lacking. However, accounts of elderberry syrup linked to Drug Induced Liver Injury and Autoimmune Hepatitis have become evident. In the latter case the overproduction of inflammatory cytokines has been considered. Depending on future incidence, proper management at the point of sale may thus require an understanding of patient history. Whilst this is possible in the pharmacy setting it is not so elsewhere.
The claimed reliability of elderberry lends itself to the appeal to antiquity as it has reportedly been used for centuries, for a host of purported reasons, as mentioned above, in addition to heart disease, gum disease, high cholesterol and obesity. The drugs.com entry for Elderberry and Sambucol are identical and include (bold mine):
It is not certain whether [Sambucol/Elderberry] is effective in treating any medical condition. Medicinal use of this product has not been approved by the FDA. This medicine should not be used in place of medication prescribed for you by your doctor.
The US Food and Drug Administration (FDA) have warned promoters of elderberry syrup, as evidenced by (for example) a September 2000 warning letter and another in August 2022, written to highlight breaches of the Federal Food, Drug and Cosmetic Act because the products advertised were “intended for use in the cure, mitigation, treatment, or prevention of disease”. The FDA does not regulate herbal supplements. In Australia the TGA accepts Sambucol Black Elderberry Cold & Flu and Sambucol Black Elderberry Cold & Flu + Pain as Listed medicines as opposed to Registered medicines.
Read more about TGA classifications here, and please remember a September 2022 TGA review of Sambucol® states, “The efficacy of the medicine was not assessed as part of this review”. Thus the term “TGA Assessed” cannot be used in relation to this product or on its label. Read more about TGA regulation of Listed medicines here. The TGA does not approve Listed medicine labels before marketing. The TGA state:
This is because we take a risk-based approach to regulation, which means higher risk medicines have more rigorous controls than lower risk medicines. However, we do require sponsors to certify that the medicine complies with all relevant regulation, and that they hold evidence that their medicine does what it says it will. Source: TGA – How we regulate medicines.
The public summary on the TGA Australian Register of Therapeutic Goods for Sambucol Black Elderberry Cold & Flu permits the following indications.
Relieve weariness/tiredness/fatigue/feeling of weakness.
Maintain/support general health and wellbeing.
Decrease/reduce/relieve common cold duration.
Helps decrease/reduce/relieve the severity of symptoms of common colds and flu.
Decrease/reduce/relieve symptoms of common colds and flu.
Label statement: If symptoms persist, talk to your health professional.
Product presentation must not imply or refer to serious forms of respiratory disorders/diseases, such as: asthma, pneumonia, COAD, COPD, influenza.
Label statement: Adults only, OR Not to be used in children under 2 years of age without medical advice (or words to that effect).
Respiratory tract infections must be qualified by ‘mild’.
Product presentation must not imply or refer to chronic fatigue syndrome.
Looking at the above it is clear the TGA have been more than generous with the allowed claims in the ARTG indications for this product. Particularly given the lack of published evidence and the absence of TGA assessment for efficacy. I don’t accept that Sambucol is clinically proven to shorten colds or boost immunity or any other claims made in sales promotion. The evidence simply isn’t there and relying on unpublished work organised and funded by Pharmacare is misleading. Whilst an impact of elderberry syrup on cold and flu symptoms is acknowledged in literature, the most common conclusion is that more research is needed. Quality human trials are still lacking.
So what might Pharmacare have planned to improve evidence in their favour? The Australian New Zealand Clinical Trials Registry, presently has the registered trial ACTRN12623000299606, last updated 7 April 2024. The title is, Determining the effectiveness of Sambucol in reducing the duration and symptoms of the common cold in children and teens. The age group is 2-17 and the aim is to use Sambucol and report on symptoms via, “a purpose-built study app ‘Sambucol Research’.” The methodology is likely to favour Pharmacare, particularly given that there is no control group. Rather, “a comparison will be made to two existing data sets”.
The first data set is reported as:
Data describing the incidence, severity and duration of different cold symptoms in children over a six-week period. (Troullos E, Baird L, Jayawardena S. Common Cold Symptoms in Children: Results of an Internet-Based Surveillance Program. J Med Internet Res. 2014 Jun 19;16(6):e144.) This study was not a randomised controlled trial or an intervention. The study observed duration and severity of colds and as such was not registered.
The second data set is “a confidential report to Pharmacare”, and is none other than the initial unpublished study that found Sambucol® “shortened colds by up to 3 days”; Rao A, Sethi M, Dick C. A double-blind, randomised, placebo-controlled study to evaluate the safety and efficacy of Sambucol liquid formulation to reduce the duration and severity of the common cold and flu symptoms in adults.
An inquest into a Kambo related fatality in Northern NSW has been suspended by NSW State Coroner Teresa O’Sullivan, who referred the matter to the Director of Public Prosecutions (DPP). This is the second inquest into a death linked to the frog poison touted as an alternative medicine, to be heard at Lismore Court House since May 2023.
Jarrad Antonovich
Evidence in this case described how Jarrad Antonovich attended the Dreaming Arts Festival in Arcoora Northern NSW, on 16 October 2021. He died of a perforated oesophagus that night. His day included a Kambo ritual at around 10am. Kambo ceremonies at the festival were being run by Cameron Kite. After the Kambo, Antonovich displayed symptoms of being very unwell, including a markedly swollen neck – an adverse reaction known to be caused by Kambo. Despite being unable to stand without support by 5pm, Mr. Antonovich was later given the psychoactive brew, ayahuasca. He died during the ayahuasca ceremony after being helped into a hall where it was to take place. Both Kambo and ayahuasca are illegal in Australia. The inquest heard from different witnesses that they believed Mr. Antonovich was in need of professional help, but they had been instructed not to interfere with anyone’s “journey”, and to trust the medicine, the shamans and the organisers. The offer to call an ambulance was made by other festival attendees, but Antonovich refused and elders “reassured” concerned onlookers.
An ambulance was not called until 11:30pm and took an hour to reach the remote location. As Jarrad Antonovich’s life ended, organiser Soulore (“Lore”) Solaris was strumming his guitar at the front of the gathering, as others in another location were being guided in CPR over radio, as they attempted to save Mr. Antonovich. When paramedics arrived Mr. Antonovich was blue in the face and dead. Ten or twenty people in the immediate area were engrossed in the ceremony and one asked paramedics to “move away from Jarred because they were interfering with his aura”. Both Kambo and ayahuasca are associated with vomiting or “purging”, as adherents refer to it. Ayahuasca induces violent and sometimes prolonged vomiting. The coroner was investigating the likelihood that vomiting caused Mr. Antonovich’s perforated oesophagus. The exact reasons behind the coroner’s decision to refer the case to the DPP cannot currently be revealed.
Lore Solaris and Cameron Kite
Dreaming Arts Festival organiser Lore Solaris, a counsellor who facilitates ayahuasca ceremonies, is presently subject to a NSW Health Care Complaints Commission interim prohibition order under the Health Care Complaints Act 1993, Section 41AA. The order reads in part:
Mr Soulore Solaris must not under any circumstances provide, or cause to be provided, any health services, either in paid employment or voluntary, to any member of the public.
Interim orders may apply “during any investigation of a complaint against a non-registered health practitioner”. The HCCC may make an interim order if:
a) it has a reasonable belief that the health practitioner has breached a code of conduct for non-registered health practitioners, and
(b) it is of the opinion that–
(i) the health practitioner poses a serious risk to the health or safety of members of the public, and
(ii) the making of an interim prohibition order is necessary to protect the health or safety of members of the public.
Jarrad Antonovich’s former partner, Patrick Santucci, gave evidence in May 2023 that Lore Solaris had called to reassure him Jarrad’s death was a “beautiful occasion”. Solaris told him that kinesiologists couldn’t find anything wrong with him. Kinesiologists utilise acupressure on points of the imaginary “meridian system” and wrongly believe the body can heal itself. They focus on “imbalances” which may be caused by a forgotten memory or even an attitude. They may use flower essence or homeopathy. There is no evidence kinesiology works. Mr. Santucci testified that Solaris told him an Aboriginal elder chanted sacred songs, “calling the spirit out of his body” and that:
[T]he koalas were making a special sound that is known to the elders when the land accepts a spirit.
Protecting Ayahuasca
Both Kite and Solaris were due to give evidence on 24 May; the day the inquest was suspended. Had they given evidence, it was expected the men would have responded to alarming statements given by other witnesses, describing attempts to cover up events and mislead police. For example Mr. Antonovich had difficulty breathing, was moaning in pain and his neck was swollen to the jaw line. Kambo practitioner Laara Cooper suggested giving him ayahuasca as this could “help shift” the Kambo induced discomfort. Consequently Antonovich was given what was described as a “not small” cup of the brew by Cameron Kite at the instruction of Solaris.
Cooper and Solaris had told ceremonial “guardians” to drive to Antonovich’s home and tell his flatmate not to mention to police the use of ayahuasca, in an attempt to “protect the medicines”. The inquest heard Cameron Kite was deeply distressed by events at the festival and told his partner at the time that Solaris and Cooper “just took over” the account given to police. Festival attendees were also told not to speak to police or paramedics about what actually happened as it may “damage the good work” being done with Kambo and ayahuasca. Antonovich was found to have ingested toxic levels of N,N-Dimethyltryptamine (DMT); ayahuasca’s most powerful psychedelic.
Both ayahuasca and Kambo are favoured as alternative medicines by neo-shamanic devotees, convinced purging “detox” experiences lead to personal growth and discovery. Logical fallacies such as appeal to antiquity, appeal to nature and an unguarded tendency toward xenocentrism, leave them vulnerable to experimentation and/or regular use of both substances. Traditional use of both can be traced back to indigenous tribes of the Amazon. Ayahuasca has a well established profile of around 70 years, as a promised cure for Western ailments, particularly those with a psychological component. It has also attracted research attention in offering an overhyped role in opiate addiction recovery. Despite some evidence suggesting it may have been used as early as 2000BC, widespread use across the Amazon was reliably established in the mid-19th century. Ayahuasca religions emerged very late in the 19th century. The Antonovich inquest heard that a Brazilian blend of Christianity and Amazonian shamanism (including drinking ayahuasca) had gained influence over The Australian Church of Ayahuasca, which had been active in the Northern Rivers region.
Kambo
Kambo has a much shorter history as a choice of alternative therapy in Western society. It gradually attracted interest after the International Association of Kambo Practitioners (IAKP) was established in 2014. Despite the flowery, earthy tones on their site, Kambo is emerging as a substance with a much higher risk profile than ayahuasca. IAKP claim:
IAKP teachers guide students to cultivate a profound comprehension and reverence for this potent natural modality. By enriching and forging connections with the intelligence and spirit of Kambo, our training courses enable practitioners to embrace personal growth, embark on a voyage of self-discovery, and engage in selfless service to others through the safe application of Kambo.
Kambo is collected from secretions of the Amazonian giant leaf frog, after “agitating” the innocent amphibian. Images suggest more than a little agitation is needed as they depict a frog tied by each leg and stretched asunder. The secretions are dried and packaged. Kambo is illegal in certain South American countries unless used in traditional indigenous practice, including Brazil. For Western ceremonies, the poison is reconstituted with water or saliva and applied to burn sites made with a smouldering stick on the arms, legs, chest or shoulder. Lucky recipients may get a dash of “dragons blood” tree sap as an antiseptic. The poison quickly makes its way into the lymphatic system then the bloodstream, and the effects begin.
Kambo lacks the psychedelic and hallucinogenic experience that ayahuasca brings. Writing for The ConversationMartin Williams notes:
Typically, the first symptoms reported are an initial rush of heat and redness of the face. Nausea and vomiting are often experienced within several minutes, accompanied by general malaise, racing heart, dizziness and swelling of the face, and sometimes an urge to defecate. Further effects include the feeling of a lump in the throat or difficulty swallowing, abdominal pain, nausea, vomiting, diarrhoea, runny nose and tears, swollen lips, eyelids or face, and occasionally a swollen tongue or throat.
Adherents claim this process rids the body of toxins, although there is no evidence supporting the claim. In 2021 the Therapeutic Goods Administration (TGA) classified Kambo as a Schedule 10 poison (page 9). They are defined as, “substances of such danger to health as to warrant prohibition of sale, supply and use”. Kambo does not have any medicinal benefit and can damage the liver, stomach and cause cardiac arrest. Visiting the IAKP website page on contraindications yields nothing but arguably useless advice; “For the latest updates and safety information relating to contraindications and cautions, please seek guidance from an IAKP trained Kambo practitioner.”
In the Natasha Lechner inquest findings, Coroner Teresa O’Sullivan referenced medical contraindications “according to the IAKP” (page 9) and observed it was unclear if these are supported by peer reviewed research. She also criticised the paucity of the IAKP information relating to “risks” and particularly IAKP training material on the risk of death. One thus wonders if the present absence of contraindications is a policy recently adopted by the IAKP. More so the IAKP Code of Ethics and Professional Practice omits any reference to the dangers of Kambo itself.
Natasha Lechner
Natasha Lechner died on 8th March 2019, following a Kambo ceremony at her home in Mullumbimby. The inquest into her death was held at Lismore in May 2023. NSW State Coroner Teresa O’Sullivan handed down her findings in February 2024. The coronial findings (PDF) provide valuable insight into the insouciance with which self proclaimed shamanic healers prepare for what is known to be a high risk “ceremony”, and the potential for tragedy that awaits vulnerable individuals drawn into this culture. This was an unnecessary death stemming from a failure to call for help.
Natasha lived with a number of chronic health issues and was unable to work. Two months before her death she had undergone a two week basic Kambo course run by the IAKP. The coroner found that the IAKP was founded by Karen Darke who has no medical qualifications. IAKP has no input from toxicologists or medical practitioners in development of their training materials. Natasha took her role as a Kambo practitioner seriously.
In 2014 Natasha met Victoria Sinclair who, as a senior Kambo practitioner used the name Maestra Victoria. Her website mentioned in the coronial finding is still available. She advertises herself extensively, including:
Victoria is a transpersonal (eco)psychologist, trauma and postcolonial theorist and plant medicine practitioner, working on a High Priestess Level of initiation, ordained through several lineages and acknowledgments and in terms of shamanic initiation and training she worked prolifically in the Free Party Scene in Europe since 1990s and has been journeying and working extensively in Central and South America and Australia since 2006.
Indeed. Ranging a little further than the inquest findings, one discovers this woman has more qualifications I’m not familiar with. Such as these “therapeutic qualifications”:
Victoria has been a Reiki practitioner since 1999 and is a Master of both Tibetan Usui Reiki and Sekhem – Seichim – Reiki. She has been teaching people globally since 2012 and has dedicated herself deeply to upgrading Sekhem teachings to help to create a Higher Pathway to Metaphysical Ethical Practitionership as part of her Dharma.
Her training background includes; Transpersonal Psychology, Non-Dual Astrology, Epigenetics, Trauma work, Pranayama, Kundalini Yoga, Plant medicines, De-colonisation and Quantum, sound and ancestral practices… She is also a plant communicator.
If you’re not convinced you’d want to be alone with Victoria when you take a frog’s defensive secretion that the TGA later classified as a schedule 10 poison, be aware that Victoria also works with indigenous groups, “around spiritual sovereignty and healing of self and eliminating planetary dis-ease to nurture higher vibrational being for the new age and evolution of homo luminus.”
Victoria Sinclair as Maestra VictoriaVictoria Sinclair as Padma Khandro
Ranging a little further allows us to meet her latest incarnation, Victoria Padma Khandro, who is offering over this year and next:
High Level Multidimensional Mentoring
Non-Dual Astrology readings and Time-line work
Soul-plan work involving fusion clearing, psychotherapy, Quantum Transfiguration, Ancestral Work, Gene Keys and Astrology zero-pointing
Therapeutic packages including ancestral work, IFS, Quantum Transfiguration, Quantum Art Therapy and sometimes in-house referrals to deepen the scope of the work.
Returning to the inquest findings, we find that before 2019 Victoria had performed Kambo ceremonies on Natasha who either paid her or provided accomodation. In March 2019 Victoria Sinclair was visiting from Ireland and was staying with Natasha at Mullumbimby. Before Sinclair arrived Natasha had reported feeling “really off”. It should be stressed that the “ceremony” was Natasha’s idea. They began the ritual by using Sananga eye drops. Sananga is another psychoactive plant extract associated with a host of unproven health benefits. Natasha administered Kambo to Sinclair who vomited, as expected, without incident.
Sinclair administered the burn wounds onto Natasha with an incense stick, then applied the Kambo. Immediately Natasha became faint and lay down. Two minutes later she sat up, grabbed Sinclair’s hand and said “this isn’t good” or “something’s not right” before passing out. Sinclair thought she might be “processing something” and held her upright for about 10 minutes as Natasha made moaning noises. Only then did she lay Natasha down in the recovery position and remove the poison from the wounds. She attempted to revive her by pouring water over her head. Then noticing goose bumps, assumed she was cold and began to massage her limbs.
Sinclair began CPR after noticing Natasha’s lips were blue. She attempted to use a mobile phone to call an ambulance. This failed as “she did not normally use mobile phones” and didn’t know the Australian emergency number. I find this deeply troubling as mobile phones allow access to dial emergency services without needing to be unlocked, or input of the specific number. As the more experienced Kambo practitioner, with a promoted reputation of travelling the global party scene, Sinclair should have known this. Natasha’s house-mate arrived home around 90 minutes after the ceremony had begun. She immediately began CPR and called an ambulance which arrived within 5 minutes. Natasha was already dead. Despite testifying she had ceased Kambo administration after Natasha’s death, Victoria Sinclair still advertises the service. The coroner specifically addressed the legalities of Sinclair’s involvement on pp. 12, 13 & 15.
As I touched on above, the coroner was critical of the IAKP training material on the risk of death. Evidence given by Sarah Morrison (aka Aisha Priya) cited the various risks discussed (page 10). On death, information for Kambo practitioners was:
Death is discussed as a risk if the water guidelines or first aid are not adhered to or if a client is contraindicated and does not disclose this or does not know they have a medical condition.
The coroner observed the incompleteness of this information and noted it does not advise even healthy people of the true risk of Kambo. Available literature and the two cases brought to the coroner’s attention led her to observe “that death can occur even where there is no pre-existing condition, or at least not one that could be possibly identified beforehand.” It is likely Natasha experienced an acute cardiac event caused by Kambo, such as cardiac arrhythmia leading to cardiac arrest or hypotension leading to cerebral hypoxia followed by respiratory arrest, as causes of her death.
Conclusion
Kambo is emerging as a significantly dangerous substance favoured by individuals interested in extreme so-called alternative medicines. It has been rapidly adopted by communities already familiar with ayahuasca, yet has a demonstrably higher risk profile. There is no scientific evidence to support the efficacy of Kambo in alleviating health problems as claimed by proponents. Nonetheless, the presence in Kambo of peptides and polypeptides with analgesic properties and affinity for opiate receptors may explain “feelings of well being and improvement of motor skills”, that users describe, and offer insight into repeated use.
Still, it is the very complex nature of active substances in the secretion that cause arterial hypotension, palpitations, cardiac arrhythmia, facial swelling (see Maestra Victoria above) and uncontrolled smooth muscle changes in the gut. To hope that shamans and self-styled practitioners of Kambo, who offer it as a means to spiritual awakening, are all capable of managing a genuine adverse reaction to the poison is futile. Use of Kambo in Western rituals is entwined with new age scam “therapies” so clearly divorced from reality as to almost beggar belief. This is not the case in the indigenous Amazon populations using Kambo.
Vulnerable individuals interested in exploring non evidence-based treatments for chronic health problems are at high risk of harm if not death from Kambo and its eager promotion. Use is likely to further increase and the self-appointed arbiters of Kambo sourcing and education, the IAKP, are manifestly ill prepared to manage present risks or to protect users.
Community education and adaptation of Harm Reduction strategies may likely prove beneficial in negating risk.
In the last post I ran through the finding by Justice Helen Rofe in the case of Fidge v Pfizer. This was the third case brought by individuals and legal representatives with strong anti-vaccination links; both ideological and active. The applicant, Dr. Julian Fidge was found to lack standing. The case was dismissed.
As I previously began to discuss, within a day of the ruling, a follower of Julian Gillespie prompted him to do some digging into Justice Helen Rofe’s career as a barrister. You see, dear reader, as a barrister Helen Rofe had represented Pfizer in cases of intellectual property and patent law between 2003 and 2006. To the antivax mindset, this was proof of corruption because she did not reveal this prior to hearing the case. As a perceived “conflict of interest” existed, Rofe should have recused herself or allowed parties to request her recusal, they argued.
Now again, I am not a lawyer and I cannot qualify the importance of the duty of disclosure in this instance. But my thoughts on this development are straightforward. Is there any evidence Justice Rofe could not have acted impartially, or did not act impartially? Or rather, did her experience make her an ideal choice to hear the case. In 1988 Helen Rofe completed a Bachelor of Science with a major in genetics. Justice Rofe states on LinkedIn:
Prior to being appointed to the Federal Court I was a commercial barrister and Queen’s Counsel specialising in science and technology related matters.
Constitutional Complaint
On 22 March 2024, PJ O’Brien and Associates filed a constitutional complaint against Justice Rofe citing not only her prior work as a barrister but also “affiliations and extended family”. According to the media release (below) Justice Rofe “concealed her connections to Pfizer and the pharmaceutical industry”.
Constitutional Complaint Media Release
I should point out that contact for the complaint, Katie Ashby-Koppens, is on the steering committee for the World Council for Health (WCH). The WCH is renowned for promoting misinformation linking COVID-19 vaccines with death. Wikipedia describes the group:
The World Council for Health is a pseudo-medical organisation dedicated to spreading misinformation to discourage COVID-19 vaccination, and promoting fake COVID-19 treatments.
The organization’s online appearance is that of a mainstream health organization. It appears to have been formed in September 2021 and its published leadership contains people which an Australian Associated Press fact check described as “figures who have promoted unfounded conspiracy theories”.
Now, better equiped to understand motivation, let us examine the complaint.
The accusations in the complaint are impressive to say the least. They require substantial “reasonable assumptions”, both numerous and convoluted. This reasoning begins by pointing out that Justice Rofe has majored in genetics, and the Fidge case involved genetics, genetically modified organisms and allegations that mRNA vaccines are GMOs. Also, we’re reminded that Justice Rofe held prior membership of the Bolton Clarke Human Research and Ethics Committee. Her cousin Sir Andrew Grimwade supported research there with grant monies from the Felton Trust. He was a member of the Felton Bequest for 50 years, and served 19 years as chairman of the bequests committee. He was a guest at the ceremony to welcome Justice Rofe to the federal court. Rofe “enjoyed a good relationship with Sir Andrew” sharing his “interest in science and scientific research”.
Sir Andrew was the great-grandson of Frederick Shepherd Grimwade who, “founded the Grimwade family pharmaceutical industry fortune in Australia”. The complaint goes on to state, Sir Andrew also “served as the honorary President of the Walter and Eliza Hall Institute (WEHI) for 14 years before retiring in 1992″ and had been on the Board since 1963. He “appears” to “have maintained a close relationship with WEHI right up until his death”, purportedly evidenced by a public guestbook obituary from WEHI.
As Australia’s leading biomedical research institute, the WEHI “may have” received billions of dollars from Australian governments. The WEHI have received $30 million from The Bill & Melinda Gates Foundation. Pfizer, BioNTech and Moderna have received six times that from the same Foundation, which has also promoted COVID-19 products. It’s “also reasonable to assume the WEHI supports all of the efforts of Mr Gates and the Bill & Melinda Gates Foundation in respect of their support of the COVID-19 products of Pfizer and Moderna.” WEHI received $13.5 million in Australian government funding for “COVID related projects”.
In mere paragraphs we’ve leapt from the failure of Justice Rofe to reveal that she had represented Pfizer some 18 to 21 years ago, to the apparent significance of her cousin’s commitment to scientific research and the involvement of the premier anti-vax enemy, Bill Gates. The complaint continues, targeting the Australian and Victorian governments’ partnership with Moderna. “It is reasonable to assume that the WEHI stands to possibly receive significant monies” from this partnership. The Victorian government has given $600,000 to WEHI as part of mRNA Victoria. “It is entirely reasonable, in light of enduring family ties and her Honour’s own scientific background and interests”, that Justice Rofe has “long been aware of the sources of funding… and the public statements in support of mRNA technologies” made by state and Commonwealth ministers and the Prime Minister.
The complaint rolls on in alleging that affiliations “reaching back four decades for her Honour personally, and over a century when extended family interests of great significance are factored in”, in fact mean a reasonable observer would accept J Rofe holds “Big Pharmaceutical interests, both domestic and international”. More so, Justice Rofe has “meaningfully and significantly assisted to protect, grow, and further establish in Australia [the interests of Pfizer]”. It is further alleged extended family ties nefariously influenced Justice Rofe’s decision-making to favour funding for WEHI, mRNA technology and “further significant sums of research monies” for both, as they’re supported by The Australian PM. Finally we reach paragraphs 42 and 43:
A reasonable observer can conclude from the above that it was more likely than not her Honour would seek to see the science and technology promoted by Pfizer and Moderna, and Australian governments, that stand to significantly benefit medical research institutes like the WEHI, survive and flourish in Australia.
Judicial proceedings of the type brought by Dr Fidge would, if successful, strike a damning blow against all the above interests, and much more.
The complaint continues with Case Implications, outlining what they believe would happen if Fidge had won the case. It not only reads like an anti-vaxxer day dream, yet reveals in black and white, the unabashed sabotage of vaccine public health initiatives and related vendettas, that this group deems justified. Australia would see injunctions and “serious criminal charges” for Pfizer and Moderna. Initiation of investigations into the “operations, processes and personnel of the OGTR, Department of Health and Aged Care” and (of course), “In particular the former Secretary of Health, Brendan Murphy due to his being responsible for provisional approval [of COVID-19 vaccines]”. In addition would be initiation of an examination to determine if the absence of GMO licences led to failure to provide proper informed consent, and medical negligence implications.
There would also be potential civil liability in the Commonwealth government for failing to enforce GMO licensing, and civil liability for Pfizer and Moderna for failing to undertake GMO licensing. The complaint also refers to “possible confirmation” of injuries and deaths caused by genetically modified properties of mRNA vaccines. Yet there is no body of work identifying such adverse outcomes. It is a misinformed notion linked to the same suite of decades old research, mRNA-critical pre-print papers, animal studies, SARS-CoV-2 infection studies and related articles that buoy this anti-vaccine belief. I’m not criticising the research, but strenuously reject the invented link to “injuries and deaths” fabricated by the anti-vaccine lobby.
Another implication of a Fidge victory, is vaccine hesitancy due to a loss of trust in Australian health authorities. Yes, they’re serious. However, vaccine hesitancy is in fact due to constant misinformation spread about vaccines, by groups such as this. Then on p. 13 we read the implication under 44 J:
The necessity to initiate many forms of clinical studies to assess the real world damage, disease, or fatal outcomes associated with the GMO products of Pfizer and Moderna, and any observed medium-to-long term disease and adverse reproductive health outcomes associated with the GMO products of Pfizer and Moderna, for those Australian citizens who were not informed they were receiving GMOs.
Astonishing. The complainants apparently believe an entire body of clinical research would evolve following a Fidge victory. One may ask, quite rightly, as to why such research into this vaccine induced disaster is not already underway. The answer being of course, that the “damage, disease and fatal outcomes” do not exist.
We then read that the complaints provided list is not exhaustive and that the implications suggested, pose severe and long lasting reputational damage and financial consequences “for all Australian political parties and their lead members in power throughout the COVID period”. Particularly for those introducing Pfizer and Moderna vaccines.
They finalise the implications by contending that these, or other implications not even listed, may have served to motivate Justice Helen Rofe to dismiss the case brought by Julian Fidge. The complaint then moves onto Judicial Conduct, and examines the Guide To Judicial Conduct with respect to J Rofe’s “failure to discharge her duty of disclosure concerning her prior dealings with Pfizer.” The complaint submits in paragraph 48:
As detailed under the section above…, her Honour Justice Rofe had significant prior dealings with Pfizer when a barrister, and through her science learnings and the interests of her extended family, significant professional and personal interest in seeing the continued success of those institutions her extended family and science colleagues had been involved with, and perhaps continue to be involved with.
The remainder of the complaint utilises the Guide to Judicial Conduct and the various summations of active bias that the complainants allege motivated J Rofe’s decision-making, in an attempt to argue she is in breach of sections of the Guide. Focusing on the principle of Impartiality and sections such as Personal Relationships, the complaint references seven “slightly different positions [reinforcing] the same common-sense view”:
Where there is a prior relationship with a party, the judicial duty is to disqualify oneself or disclose the relationship before all the parties. If in doubt about disqualification, disclose the relationship before all the parties and invite submissions.
Again, impartiality should be determined by “a fair-minded lay observer who might reasonably apprehend that the judge might not [be impartial]”. Whilst perception of bias and conflict of interest sufficient for disqualification from a case “is to be judged by the perception of a reasonable well-informed observer”. Parties should be informed by the judge of facts which might give rise to perceptions of bias, but the judge must decide on the appropriateness to sit on a case.
Conclusion
For this author, looking through the complaint is like reading any text peppered with the red flags of anti-vaccine beliefs combined with an entrenched distrust of medical, legal and government authority. I can see nothing wrong with the legal team of Julian Fidge raising concerns over Justice Rofe’s failure to disclose her past history representing Pfizer. I don’t believe there’s much substance to it but respect their right to raise concerns. However, the constitutional complaint itself relies on typical anti-vax tropes such as distrusting J Rofe’s respect for science and research, and her affiliations with individuals or organisations linked to vaccine technology and/or its funding. Indeed the complaint made a number of connections that whilst exhaustive, are difficult to respect, much less accept. To argue that J Rofe acted with corrupt intent, primarily to avoid the dawn of the post Fidge-victory era as the complaint described it, is simply fantastic.
I can only conclude by wishing Justice Helen Rofe all the very best.
Professional Conduct Rules for Lawyers
As a footnote, it’s worth pausing to consider that lawyers and solicitors are also subject to professional conduct rules. Katie Ashby-Koppens and Peter O’Brien & Associates must keep in mind their duty to the court and the administration of justice.
Lacking professional distance from your client (or their cause) risks distracting you from this duty, which is paramount and prevails to the extent of inconsistency with any other duty. Your objectivity, your independence and your forensic judgement – on which the court relies – may be reduced.
The duty to avoid any compromise to integrity and professional independence:
Your integrity and trustworthiness are fundamental to your reputation as a lawyer and to your relationships with clients and other parties in the justice system. When a lawyer fails to act with integrity because their professional boundaries are compromised, the integrity of the justice system as a whole is undermined.
Critical overdose events at three Australian dance parties in January this year, have led to more calls for Pill Testing (PT) to be introduced as part of our nation’s effective Harm Minimisation drug policy. Harm Minimisation consists of three prongs: Demand Reduction, Supply Reduction and Harm Reduction.
Strong evidence
Pill testing is an evidence-based, harm reduction initiative backed in peer reviewed literature. It reduces drug harms and protects the health of those who access the service. Whilst Australian drug markets are uniquely sourced and specifically affect Australians, Harm Reduction Australia cites Harm Reduction International, in answering the question, What is harm reduction?
Harm reduction refers to policies, programmes and practices that aim to minimise negative health, social and legal impacts associated with drug use, drug policies and drug laws. Harm reduction is grounded in justice and human rights. It focuses on positive change and on working with people without judgement, coercion, discrimination, or requiring that they stop using drugs as a precondition of support.
PT has been demonstrated via live trials at Canberra’s Groovin The Moo festival in 2018 and 2019, to be effective in positively changing behaviour related to drug use. The trials were conducted by Pill Testing Australia, and resulting evidence greatly contributed to the fixed-site testing facility CanTEST, an ongoing trial in Canberra, introduced in July 2022. Indicating the controversy of PT, days before a third dance festival trial was scheduled to begin in 2022, Pill Testing Australia had public liability insurance withdrawn, without explanation.
A 2019 election study found two thirds of Australians support PT at music festivals. Examining deaths, PT initiatives, the success of harm reduction and drug user responses, Andrew Groves wrote in The Harm Reduction Journal in 2018:
Using a theoretical frame of pragmatism and drawing from national and international research evidence, this paper recommends the integration of pill testing into Australia’s harm minimisation strategy.
Australia’s Alcohol and Drug Foundation have published an excellent summary of the evidence supporting PT, and provide data on its successful international uptake. They also point out that public health experts have demonstrated support for PT. These include:
In February 2023, directly citing the success in Canberra, the QLD Palaszczuk government announced plans to develop Drug Checking at fixed and mobile sites. This very shortly followed the state’s plans to reduce penalties for illicit drug possession, including heroin, ice and cocaine. More so, use of the term “drug-checking” is more realistic, inclusive and in line with international practice, as summed up in this opening paragraph from the QLD Network of Alcohol and other Drug Agencies (QNADA):
Drug checking – also sometimes referred to as ‘pill testing’ – involves members of the public voluntarily providing samples of suspected illicit substances they are intending to consume (e.g. tablets, capsules, powders, tabs/blotter paper etc) for chemical analysis.
Test results are provided back to the individual by health professionals as part of a personalised health and harm reduction intervention. The purpose of the intervention is to increase the person’s awareness of the risks associated with the substance with the aim of effecting behaviour changes that result in fewer harms or incidences of drug-related death.
In September last year the QLD government sought private providers to offer plans for two fixed drug-checking sites and mobile services. Of course, great strides like this rarely escape unhelpful politicisation. It was impossible to miss that when announced, the decision was called “soft on drugs” by QLD opposition health spokeswoman, and registered nurse, Ros Bates. It’s been a long time since I’ve heard that phrase used seriously.
Victoria
It is Victoria, to where we must turn our attention to partly examine the recent overdose events. RACGP reported eight people, most in their 20s were intubated and placed in induced comas after MDMA overdose at the Hardmission dance party in early January. Jollyon Attwooll reported:
Chair of RACGP Specific Interests Addiction Medicine Dr Hester Wilson described the introduction of festival pill testing as ‘a no-brainer’. ‘[Pill testing] actually does change people’s behaviour, and therefore it makes it safer,’ she told newsGP. Dr Wilson said that pill testing is ‘not a silver bullet’ but should be used as part of a range of measures to address drug use.
Following the Hardmission OD events, two women were taken to hospital on January 12 after suspected drug use at Juicy Fest. Current Victorian Premier Jacinta Allan initially stated she had no plans to introduce PT. Not long after, Allan advised that she would seek more information from the health department. The Premier sensibly observed:
I think it’s important to examine the evidence and advice and consider that in the policy setting that we have across all of our alcohol and drug policy measures, which is taking a harm minimisation approach, looking at the safety of people going to events.
The ACT
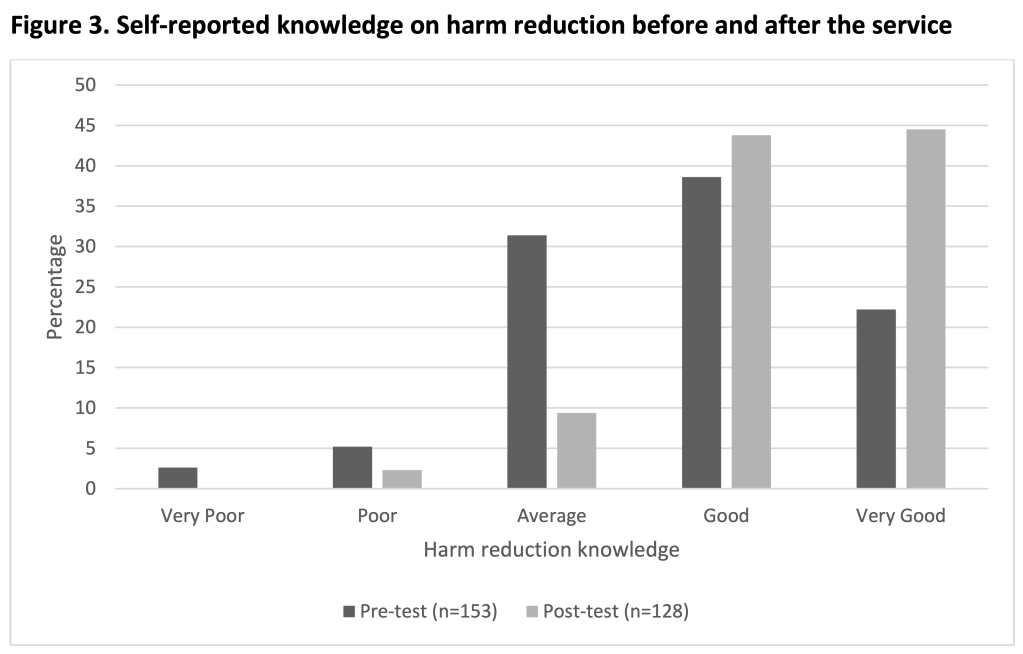
The evaluation document of the 2019 ACT Pill Testing trial is a lengthy read, with confirmation of Dr. Hester Wilson’s words coming through in data and discussion. I won’t copy/paste quotes from patrons who attended the PT facility, but I do recommend skimming through to appreciate that PT, like other harm reduction initiatives, changes drug users behaviour for the better. I did appreciate the graphs on self-reported knowledge of harm reduction before and after having a drug tested. Likewise, when it came to choice of information source, positive changes are evident.
Detailed explanation of the slides below can be found at section/s 6.1 (fig. 1), 6.4.1. (fig. 3) and 6.4.5. (fig.4).
Sydney
At the end of January a challenging scenario unfolded at Sydney’s HTID festival. Having taken what he thought was MDMA, an attendee fell unwell. Ultimately he responded to naloxone, a drug that reverses the effect of opioids. He had taken a tablet cut with nitazene, which is a synthetic opioid reported as “stronger than” fentanyl or heroin. Health workers and members of drug safety volunteers DanceWize, worked to advise the crowd. No doubt they saved lives. It turned out others from around Sydney had been hospitalised that weekend. One pill analysed, contained nitazene and no MDMA. Guardian reported:
Chris Gough, chief executive of the nation’s only pill testing venue in Canberra, said the detection of nitazenes in pills sold as MDMA showed the need for similar services in other states.
“In this case, where a nitazene has been sold as MDMA and therefore people are completely unprepared and potentially opioid naive, the risk of overdose is extreme,” said Gough, who is the executive director of the Canberra Alliance for Harm Minimisation and Advocacy.
“As we have now seen nitazenes in several jurisdictions in Australia it is time to act swiftly to provide drug-checking services throughout Australia so that we can respond to these drug trends as they emerge and thereby save lives and inform the community.”
Canberra
Saving lives is far more about probability than possibility. Indeed that’s been the case with MDMA overdose, MDMA pills cut with N-ethylpentalone or other adulterants. Early last year the Canberra walk-in site CanTEST discovered a pill cut with metonitazene; a synthetic opioid with a potency up to 200 times that of morphine. The owner chose to dispose of the drug on site. In January this year, ANU chemists made an Australia-first discovery of three new recreational drugs. All came from preparations sold as something else. CanTEST staff were able to discern the drugs were not what they were supposed to be, but tests were inconclusive. They were however, able to warn the community. One substance thought to be a derivative of Ritalin was in fact a new variant of cathinone, commonly known as “bath-salts”.
ACT Health have also developed a comprehensive document for festival planners. The Festivals Pill Testing Policy, examines PT options as a service available for festival attendees and how it relates to harm minimisation. Advice on general and specific health and safety measures, the importance of peer support, relaxation areas, emergency services and how PT works with providers and the event itself, is only part of the clear information presented.
Coronial support
A number of fatalities, and the fact that PT promotes positive decision making led to multiple calls to introduce the practice as a policy initiative. Over the last six years, four state coroners have spoken out. A 2020 inquest into five deaths from July 2016 to January 2017, led Victorian coroner Pares Spanos to urge the Victorian government to “urgently” introduce drug checking and a system to warn the community about dangerous substances sold as MDMA. The males aged from 17 to 32 died in a variety of tragic ways after taking what they believed was a modest dose of MDMA. Autopsy revealed the substances 25C-NBOMe and 4-Fluoroamphetamine in their systems. The cluster was discovered after 20 hospitalisations stemming from the Chapel Street nightclub district in January 2017. Victoria Police knew of the dangerous drug’s presence and later defended their decision to not warn the community.
In September last year, Victorian coroner John Cain also called on the government to introduce PT after the death of a man from an MDMA overdose in March 2022. The man had been observed taking a Blue Punisher, a pill with dangerously high levels of MDMA. He was admitted to the Royal Melbourne with brain swelling and multi-organ failure and died four days later. In his findings Cain wrote:
It is impossible to know whether, had a drug checking service existed, [the man] would have submitted a sample of an MDMA pill for testing before taking it at Karnival […] Notwithstanding this, a drug-checking service would have at least created the opportunity for him to do so, and for him to receive tailored harm reduction information from the drug-checking facility.
It is likewise impossible to know whether, had [the man] been provided information of this type, he would have changed his drug consumption behaviour; but likewise, in the absence of a drug checking service, this was not a possible outcome.
Politics
NSW and Victoria have established histories of resisting PT. After the death of a 26 year old at a Sydney music festival in February 2023, Dominic Perrottet mused about his government’s inquiry into methamphetamine and, rejecting any notion of PT offered a most unhelpful contribution:
But my clear message to people right across NSW [is] stay safe, and don’t take drugs and you will be safe.
Associate Professor David Caldicott, one of the driving minds behind CanTEST, suggested Perrottet had engaged in “magical thinking”. In Victoria we have the legacy of Dan Andrews who, citing the demonstrably false [HRJ] claim that PT encouraged pill taking (a belief favoured by Craig Kelly), insisted that under his leadership PT would never be introduced. The state opposition has been steadily opposed to harm reduction measures for conservative political reasons. Ignoring evidence, consecutive opposition leaders have opposed Safe Injecting Facilities and PT alike. I do acknowledge however, that the Victorian opposition has lobbied the state government for more effective emergency drug alert systems.
Recent research
A recent paper Drug-related deaths at Australian music festivals, was published last month in the International Journal of Drug Policy. Examination of the National Coronial Information System (NCIS) yielded the following results about fatalities at music festivals between 2000 and 2019:
There were 64 deaths, of which most involved males (73.4%) aged in their mid-20s (range 15-50 years). Drug toxicity was the most common primary cause of death (46.9%) followed by external injuries (37.5%). The drug most commonly detected or reported as being used was MDMA (65.6%), followed by alcohol (46.9%) and cannabis (17.2%), with most cases reporting the use of two or more drugs (including alcohol) and 36% reporting a history of drug misuse in the coroner’s findings. Most deaths were unintentional, with less than a fifth of cases (17.2%) involving intentional self-harm. Clinical intervention was involved in 64.1% of cases and most festivals occurred in inner city locations (59.4%).
There are complex factors identified in the paper, such as inner city events and multi-day events being more likely to be the site of a fatality. This may reflect policing strategies and the need for harm reduction strategies, respectively. Alcohol is known to be a compounding factor and its use is clearly identified as the second most prevalent substance (see bar graph below). Males are more likely to drink and use MDMA and this is reflected in them making up just under three quarters of deaths. Of 2000 festival goers surveyed, 52% were male. Poor decision making associated with alcohol intake is always a potential factor with illicit drug use.
Total number of drug-related deaths, deaths primarily attributed to MDMA, and deaths primarily attributed to alcohol, at music festivals in Australia by year ranges (n=64)
Harm reduction flexibility
What I took away from this paper was the recommendation that a range of harm reduction measures would each have something to offer in solving this persistent, multifactorial problem. More so, understanding data yielded by such research is vital to establishing the correct harm reduction approach for the Australian population in these instances. In conclusion, the authors write:
Harm reduction strategies such as roving first aid volunteers, mobile medical care, spaces to rest, hydration stations, and drug checking services, may best address some of the risks associated with illicit drug use at festivals, in addition to increased consumer education and awareness. It is important to understand the factors involved in these incidents in order to inform policies around harm reduction and law enforcement at music festivals in future to prevent further deaths.
Just as is the case with injecting facilities, substance checking is a successful, global health policy dynamic. Like all aspects of harm reduction the evidence supporting it is strong, persisting through variations specific to where it is a reality. In Canada, Toronto ran a comprehensive trial from 2019 to 2023. Switzerland has had drug checking available since the 1990’s. Now in a number of cities, the past decade saw a 250% increase in samples tested there. The UK has drug checking services, as does New Zealand.
Despite certain dynamics in NSW and Victoria leaving state governments out of touch with most Australians, there are cabinet ministers and cross-bench teams respectively, raising awareness and pushing for change in each state. When we look at arguments for and against PT, it appears arguments against, lack realistic substance. Indeed these documents recognise the importance of harm minimisation and its place in the National Drug Strategy. The most comprehensive argument “against” is criticism of the limitations of on-site drug checking, compared to laboratory testing. This is well understood and has been directly addressed by Dr. Monica Barratt. Of course the inevitable case that flexible harm reduction measures encourage or create the illusion of safety around illicit drugs is always mentioned. The evidence simply does not support this.
Drug Free Australia
This brings us to the anti-drug lobby. Certain groups contend that law enforcement and zero tolerance are superior in managing drug related harms. Stridently anti Harm Minimisation, they promote the ideology of a drug free world, consistently undermining evidence. In fact my own interest in the anti-vaccination lobby, began in 2009 and I was struck by similarities between their tactics, and those of the more lethal anti-drug lobby, I was long familiar with.
One group, Drug Free Australia (DFA), operate similarly to The Australian Vaccination-risks Network (AVN). DFA aggressively lobby government and an unsuspecting public, frequently using alarming irrelevant information. They attack the media, use meaningless or decontextualised data to dispute published evidence or argue that acknowledging a need for more research, reveals lack of any research. DFA dismiss harm reduction techniques by highlighting the ongoing presence of harm (eg; MDMA has caused deaths, thus no rationale for PT exists) or blame harm reduction for drug user risk-taking, and the familiar contention that PT “green lights” the taking of MDMA.
Such contentions stem from ignoring that high risk behaviour via illicit drug use continues all day, every day in Australia. Harm reduction aims to reduce the harms associated with this behaviour. It provides education, promotes safe choices, saves our health-system money, and yes, saves lives. One way DFA contend PT actually kills, is by misrepresenting the PT card system. A drug found to contain what the owner expected is “white-carded”; as is say, an MDMA pill free of any pollutant. Yet, MDMA causes most overdoses say DFA, so a white-card result must be potentially lethal. Well, no. The drug is what the person expected. Not double or five times the amount. So the patron may take the drug they bought and, remembering the slide show above, will henceforth access reputable information on harm reduction.
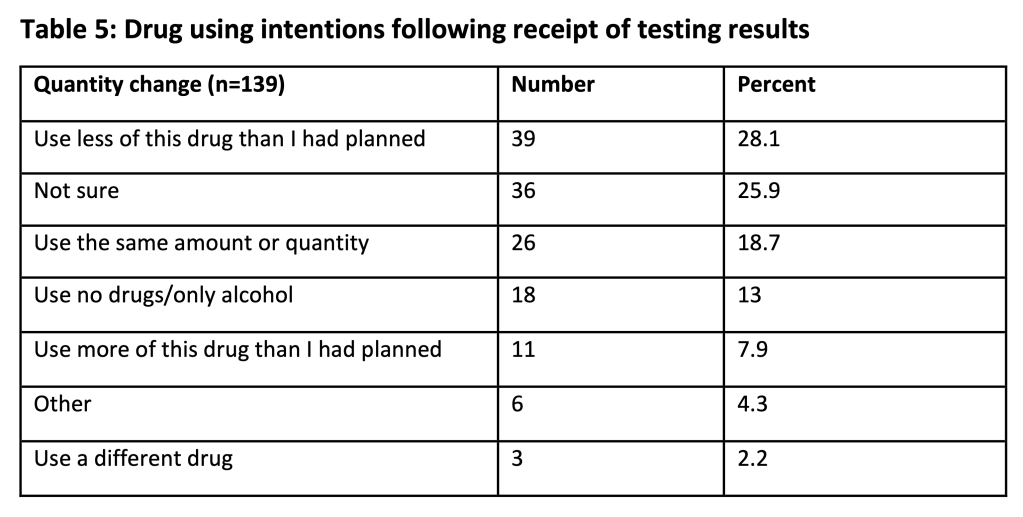
Those slides are from the ACT Pill Testing Trial 2019. DFA attack those findings in a deceptive piece, arguing the opposite to accepted findings. On page 7, they selectively quote from evaluators who discuss that someone who discovers that the drug is what they thought, “…are likely to take as much or more” (p.33). And that “…concordance between expectation and identification is associated with stable or increased intention to take a substance” (p.34). DFA use this to extrapolate to the conclusion that PT will lead to more use and thus, more death. This requires logical fallacies: Decontextualisation and cherry picking of data. Reading the full sentences and paragraphs in which those terms appear leaves the reader with a positive, not negative view of the evaluation. See pp. 33-34, and consider Table 5 from p. 32, below:
When read in context we see that patrons intent to use drugs did not dramatically change, but their intent to engage in harm reduction behaviour notably increased. Eg, also on p.33 (bold mine); Many interviewees reported that the quantity of drugs that they intended to use did not change after testing, as the drug was identified to be what they expected. And, Many interview patrons indicated that their intention to use did not change, but their intention to engage in harm reduction behaviours did increase. Also, this and other evaluations have found non-concordance between patrons’ expectation of what a substance is and what a substance is identified to be, commonly leads to reduced intention to take that substance.
So, the comment pulled from p. 33 by DFA, omits crucial clarification from the evaluation. Some was printed on the same page, just two paragraphs above. For example:
Interview data suggests that this group were looking for confirmation of the contents of the presented drug, and information about how to reduce potential harms. Many interview patrons indicated that their intention to use did not change, but their intention to engage in harm reduction behaviours increased.
Prior research also indicates concordance is associated with an increased likelihood of taking the drug, and non-concordance with a decreased likelihood (Valente: 2019, and Measham: 2018). More so, the evaluators stress that modification of drug consumption can’t be measured alone. Contextual factors, such as type of festival influencing available drugs, need to be considered during interpretation of results and future study design.
Finally, the insistence by DFA that MDMA, not impurities, lead to most fatal overdoses is fashioned only to discredit PT. Still, five deaths in the six months leading up to January 2017 and investigated by Coroner Pares Spanos involved 25C-NBOMe and 4-Fluoroamphetamine. Recent discovery of potent opioids nitazene and metonitazene raise further concern. N-ethylpentalone is regularly found in so-called MDMA pills. But why get hung up on MDMA? Drug checking can check any drugs and CanTEST discovered three unknown substances, later confirmed at ANU. This is how a new type of cathinone (bath salt) was found. Supposed ketamine was actually a new type of benzylpiperazine (BZP) stimulant. The third find was propylphenidine.
Conclusion
Pill testing or drug checking is a harm reduction measure supported by consistent evidence in peer reviewed literature. Globally, where introduced, it has demonstrated success and improved understanding of behaviour. It is supported by most Australians, where valuable data has been gathered from on-site testing at music festivals, and the fixed site CanTEST, in Canberra.
This has expanded the nation’s understanding of drug user insight into, and uptake of harm reduction dynamics. QLD is the most recent state to confirm permanent drug testing. Arguments against the initiative are morally subjective and/or deceptive, leading to their swift deconstruction.
Drug checking saves lives and is supported by public health experts across Australia. As a dynamic, expanding, harm reduction initiative, it should be introduced nation-wide into Australia’s harm minimisation strategy.
♠︎ ♠︎ ♠︎ ♠︎
Originally published as Pill Testing: The harm reduction initiative supported by strong evidence