Former editor of the Medical Journal of Australia and GP Dr Annette Katelaris interviews Dr. Ken Harvey.
Dr. Harvey originally graduated from the University of Melbourne. Initially specialising in infectious disease and medical microbiology Ken’s interest in antibiotic resistance led to a study of the forces that drive prescription. Ken moved to the School of Public Health at La Trobe University to continue his work on medicinal drug policy.
He now holds the position of Adjunct Associate Professor in the School of Public Health at La Trobe.
INTERVIEW – CAMs regulation and pharmaceutical industry influence – Assoc Prof Ken Harvey – Obserations
Noted public health advocate Associate Professor Ken Harvey on what’s lacking in regulating complementary medicines, and the influence of the pharmaceutical industry on ‘the hand that writes the script’.
Ken talks about his extensive role in prodding Australia’s regulator of complementary medicines and shortfalls in the present system for regulating these “listed” therapeutic products. He is also asked about the personal impact of holding shonky products, advertising and ultimately – dishonest, unforgiving individuals – to account. Ken’s interest in information technology makes him a welcome source of advice to overhaul the TGA’s Electronic Listing Facility.
For a self confessed “stubborn bastard” in chasing blatant advertising breaches, it’s clear that Australian consumers are in Ken’s debt. Ken holds life membership of the Australian Consumers Association, Choice, and is also a member of their Policy Advisory Group. Dr. Harvey is Chair of Health Action International, Asia Pacific (HAIAP). He was a member of the WHO expert group that drafted their Ethical Criteria for Medicinal Drug Promotion. [22 page PDF]
INTERVIEW AUDIO
Or direct download MP3 here. 21 min 13 sec. 21.4 MB
The misinformation peddled by antivaccinationists over the years will be underscored as just that. Misinformation. From ridiculous to dangerous these snippets of so-called wisdom have included claiming “measles” means “a gift from a goddess” in ancient Sanskrit, to measles being the cause of the growth spurt that happens to correlate with the most common age for childhood infection.
In the first instance a check of the link to Sitala Mataji – originally the smallpox goddess worshipped in Pakistan, Northern India, Nepal and Bangladesh – shows the divine influence to be malignant. Just as Sitala was burned by a carelessly forgotten stove, she randomly picks children in anger and burns them from within to punish the mortal.
Meryl Dorey of the Australian Vaccination Network argues that as just one of the diseases that have “beneficial aspects… prevention may not necessarily be in the best interests of the child”.
Called “gift from a goddess” in Sanskrit measles can help to mature the immune system, may help to prevent auto-immune illnesses such as cancer, asthma and allergies later in life
In reality the Sanskrit word, “masuurikaa” translates variously as smallpox, measles, eruption of lentil shaped pustules, lentil, and procuress (female procurer). There is absolutely no evidence that infection with wild measles primes the immune system against cancers or allergies. Such claims belong firmly alongside the lie that certain potentially fatal and disabling diseases are “rights of passage”. Regarding pertussis and measles Dorey famously informed a national T.V. audience:
My mother used to put me with all the neighbourhood kids when they got these diseases so we would get them and get them over with and be immune. And there was no fear, there was no worry about it. We just got them, and we were supposed to get them and we did, and we were healthier for them. Now we have a medical community that’s saying if you get measles, if you get whooping cough you’re going to die from it. Well, where is the information from that? You didn’t die from it thirty years ago and you’re not going to die from it today.
In fact with measles the risk of encephalitis is at least 1,000 times greater from measles infection than from vaccination. Prior to the success of mass vaccination:
Measles was once a common childhood disease in Australia, and medical practitioners were well acquainted with the “fever, generalised maculopapular rash, cough and conjunctivitis” syndrome that equated to a measles diagnosis. Measles complications, particularly bronchopneumonia and otitis media in children, were commonplace. With so many cases in the community, relatively uncommon severe complications, including acute encephalitis (1 in 2000 cases), subacute sclerosing panencephalitis (1 in 25 000 cases), and death, were also encountered.
There is nothing “marvellous” about measles as suggested by a despicably misleading book. Aside from the sliding scale of disability cruelly dealt by encephalitis one or two fatalities per thousand infections is normal.
The overwhelmingly positive impact of mass vaccination can be seen in the catch up programme documented here as The Australian Measles Control Campaign, 1998. There are no conflicts of interest declared by the 12 authors.
The Abstract reads:
The 1998 Australian Measles Campaign had as it’s aim improved immunization coverage among children aged 1-12 years and, in the longer term, prevention of measles epidemics. The campaign included mass school based measles-mumps-rubella vaccination of children aged 5-12 years and a catchup program for preschool children. More than 1.33 million children aged 5-12 years were vaccinated at school: serological monitoring showed that 94% of such children were protected after the campaign, whereas only 84% had been protected previously.
Among preschool children aged 1-3.5 years the corresponding levels of protection were 89% and 82%. During the six months following the campaign there was a marked reduction in the number of measles cases in children in targetted age groups.
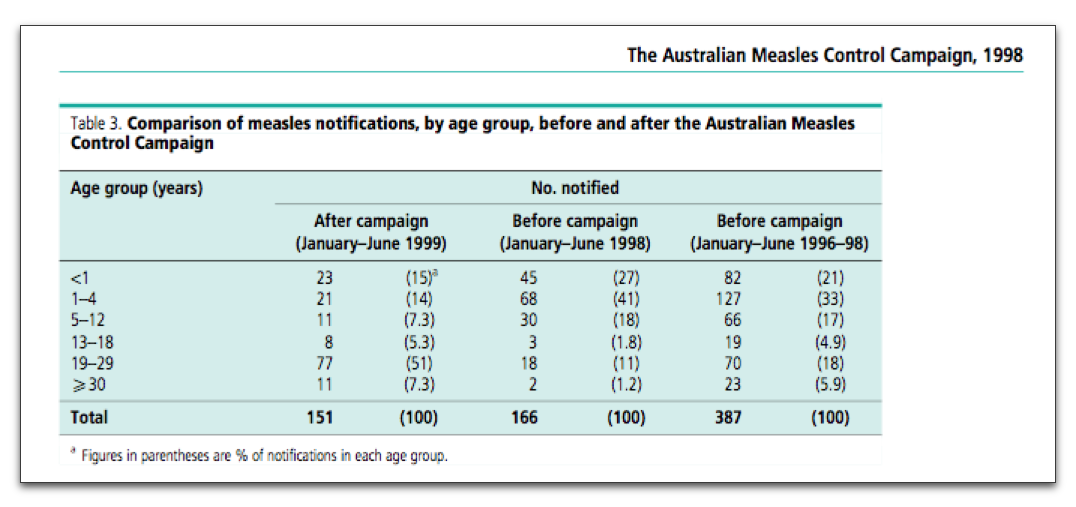
Six pages in on page 887 of the Bulletin of The World Health Organisation 2001, 79 (9), we find this table:
The authors note that whilst there was no immediate reduction in the number of cases in the six months following the campaign, there was a notable reduction in the age groups targetted by the campaign. Following 1.7 million MMR doses during the campaign, there were 89 Adverse Events Following Immunisation. 80 children followed up recovered without sequelae. Nine could not be followed up due to confidentiality restraints associated with ADRAC. The benefits were not seen in “untargetted” 12-18 year olds.
As one of the largest initiatives in Australia’s immunisation history, the MCC was deemed demonstrably effective. The authors wrote:
Each of the studies in this evaluation confirmed that the campaign was highly successful, particularly among preschool and primary-school children.
Graphed data including the impact of the MCC can also be seen here (Victoria 1962 – 2004) and here (Australia 1991 – 2011). The profound impact of the introduction of a second dose in 1994 is also clear in the second graph.
The two clusters in Victoria currently reflect one distinct arrival from overseas and a source traced to a domestic flight. A disturbing case in S.A. in August 2011 resulted in two distinct warnings stemming from just one overseas arrival. The only reliable defence against jet-setting viruses and wide scale outbreaks is herd immunity.
The need for ensuring oneself is vaccinated against measles goes without saying. Particularly as exposure to someone emigrating or returning from a part of the world where measles is poorly controlled is quite simply a matter of chance. In Measles Immunity in Young Australian Adults, Gidding and Gilbert write in Conclusion:
Based on the most recent national serosurvey data available, there are 2 cohorts with levels of immunity below 90 per cent — those aged under 6 years in 1999 (born in 1994-1999) and those aged 18-22 years in 1996-98 (born in 1974-1980). Only persons aged 30 years and over in 1996-98 (ie born before measles vaccine was available) had immunity levels above 95 per cent.
These results indicate the ongoing need to improve vaccine uptake in infants and suggest that a vaccination campaign targeting young adults would be beneficial.
If we wish to attenuate measles outbreaks to state level – indeed Victoria itself – we can examine a 2005 review by Becker et al. Monitoring measles elimination in Victoria, brings into sharp focus how damaging a drop in herd immunity can be, given that outbreaks – including this one – begin with importation of the virus.
The University of QLD authors sought to use “evidence from outbreak data that Victoria has achieved, and is maintaining, elimination of measles”. They wrote:
Conclusions: The data provide strong evidence that Victoria has maintained elimination of measles over the period 1998 to mid-2003. There is scope to improve the immunisation coverage. It is not clear how much outbreak intervention is contributing to the success in achieving apparent elimination.
Implications: To prevent importations from causing a major epidemic of measles, Victoria must maintain its immunisation coverage and outbreak control at current levels, or better. It is important to monitor the control of measles even when elimination is achieved.
Time and again we see the need to maintain herd immunity via mass vaccination. Lyn Gilbert wrote in June 2011 that researchers have presented evidence that measles has been “effectively eliminated” from Australia, “as well as from Finland, the United States, South Korea, Mexico, Brazil, Canada and Cuba”.
Elimination of measles is a viable goal for a number of developed nations. The stability of elimination has slipped further from our grasp for reasons including increased importation, socioeconomic realities and the feverish efforts of antivaccinationists. Measles is a potentially fatal and entirely preventable disease that also leaves many sufferers with lifelong disability.
It’s a public health disgrace that the measles virus can arrive in Australia to meet willing hosts who have been misled into risking their own or their children’s quality of life. That this is compounded by a demographic that experiences poverty and social trauma is a negative dynamic that health authorities should strive to rectify.
It is important that a calm measured approach is taken in educating the community about the dangers of measles and effectiveness of MMR immunisation. Also, strict and lasting penalties need to be dealt to homeopaths and chiropractors (to name just a few peddlers of alternatives to medicine) who profit from risking the lives of innocent Aussies.
The wrath of the goddess Sitala Mataji is something Aussies can do without.
Vaccination is now recognised as one of the most successful and effective public health interventions for saving lives and promoting good health. Prevention is a key goal in healthcare and the ability of vaccines to prevent illness and death associated with many serious diseases is one of the success stories of scientific innovation
♦♦ Dr. James Reilly, Minister for Health, Ireland ♦♦
Last month, during European Immunisation Week (April 21st – April 27th), Ireland launched a rather clever campaign to help remind the public of how crucial national immunisation programmes are. More importantly it included how vital it is to complete a vaccine schedule. A schedule may be one or a varied series of vaccinations, immunisations, shots and/or doses.
These may be had once, twice, three or even more times, at different ages, when exact or different time-periods have elapsed, and at which the same or different amounts of vaccine is given. Boosters can be scheduled or even recommended for other members of the family. All this depends almost exclusively on the vaccine under consideration.
So it seems that the development of immunity is remarkably complex. It is not difficult but it’s complexity can be gleaned through the above and use of terms such as “partial immunity”, “fully immune”, “waning immunity”, “herd immunity”, etc. Thus it’s very important to take the advice of your GP, doctor or local health authority rather than try to “research” the topic yourself.
The development of immunity may be complex, but we do know the development of vaccines is perhaps the greatest advance of modern medicine. In fact rather than getting bogged down in the copious amount of information regarding vaccines one could simply observe that Every Vaccine is a Little Victory.
Which brings us to the campaign itself launched last month in Ireland. Check out the video below. Chaps: you’re permitted to chuckle, smile, use words like “cool”, “nice kid”, suggest it’s a “top idea” and so on. Ladies: you may “Squeeee!, use words like “cute”, “gorgeous”, “Awwwwww”, etcetera. Do pass it around, all.
No matter how you react I trust you agree it’s a good idea. There is so much information and misinformation about vaccination, that purporting to “research” the topic and decide against vaccination is likely to involve denial of evidence. Indeed, quite a lot of evidence denial goes into rejecting vaccination.
Similarly, it’s going to prove rather challenging to suavely explain to ones mates and relatives the immunodynamics behind ones child’s third MMR vaccine. One might also look overly ambitious mounting a dinner discussion based on why it is quite safe to “complete the MMR schedule, chaps, in temporal proximity to this seasons influenza vaccine”.
Or reassure the gang over coffee that Janine can have faith in the immunogenicity of the live-attenuated influenza vaccine (LAIV) taken concurrently with the twins’ 56 week MMR dose. Perhaps, what’s really on everybody’s mind is the GMP standards as they apply to the reconstitution of vaccine diluent preparations?
Umm… No. As stated the amount of information out there is truly copious. Only the anti-vaccine lobby can keep a straight face whilst claiming to grasp the entirety of vaccine science and rewrite it’s conclusions at the same time. Perhaps they have drastic inside information on reconstituting vaccine diluent preparations?! Or rather, perhaps their unique way of getting attention is just a unique way of… getting attention.
For the rest of us, given that it’s far better to accept the word of qualified experts who overwhelmingly support vaccination, the word on the street is that Every Vaccine is a Little Victory. Presently it’s vital to remember this. The South of Wales in the UK is in the grip of a measles epidemic. Well over 1,100 cases and a frantic MMR catch-up programme has left the anti-vaccination lobby with all the charm of a malignant Chucky the Court Jester.
With rising conscientious objection in the developed world, vaccine preventable diseases once thought all but eradicated are making a firm comeback. In the developing world, communities and parents are risking their lives to access vaccines for their children.
It was with certain purpose last month in Dublin then that Dr. James Reilly the Irish Minister for Health addressed a crowd gathered at the Royal College of Physicians, Trinity College. Health News Ireland reported that, Reilly observed:
“Vaccination is now recognised as one of the most successful and effective public health interventions for saving lives and promoting good health,” he told the gathering in the prestigious Royal College of Physicians, which nestles in the shadow of Trinity College.
“Prevention is a key goal in healthcare and the ability of vaccines to prevent illness and death associated with many serious diseases is one of the success stories of scientific innovation”.
He appeared to have no time for the detractors, the nay-sayers; or the ‘scattered thinking’ brigade, as he dubbed them.
The vast majority of side-effects are minor and temporary, such as a sore arm or mild fever and have nothing to do with the infectious disease against which the immunisation is directed. New vaccines go through a rigorous testing in development and approval phases in Europe to make sure they are safe. The European Medicines Agency also monitors any adverse side-effects that might occur after the medicine is licensed.
In Ireland the National Immunisation Advisory Committee advises the “Chief Medical Officer in the Department of Health on immunisation-related and vaccine matters”. Their responsibility to the Department of Health is to ensure the ability “to enable evidence-based immunisation related policy decisions”.
One possibility in view of the order to change its name within two months or face deregistration may at least save on logos and letterhead acronyms. In an interview today on 2UE NSW Minister for Fair Trading, Anthony Roberts observed that such groups were “nut-jobs” (a technical term he assured listeners) who frequently also offer the benefits of positive vibes and living on fresh air.
Yes, we’ve noticed.
Perhaps not endearing in the eyes of some but Australian Vaccination Nut-jobs is certainly a darn sight more accurate than any title conveying expertise.
Let’s face it. Anthony Roberts may be firm, but he’s also fair. The AVN could become The AVN. Which would also work for the “Hate Group”, Stop The AVN.
James – The Amazing – Randi chats to Jon Faine and Stella Young on ABC 774.
The occasion was The Conversation Hour on Friday November 30th in Melbourne. Randi was in Melbourne for the Australian Skeptics National Convention for 2012. Join in as Randi, Jon and Stella revisit some of Randi’s memories of earlier visits, including the always-asked-about Don Lane episode.