
The most dangerous aspect of drug use is that the chemical becomes the centre of life, leads to physical debilitation after tolerance is reached, and no amount of drug produces the necessary euphoria – only coma or suicide are left
– Herschel Mills Baker (Drug Free Australia)
“Suicide/Schizophrenia: Consequences of acute and chronic cannabis use” –
A recent thread on Facebook gave me cause to reflect upon the impact that the anti-drug lobby has had upon community perception of evidence specific to cannabis, its use, abuse and potential.
This perception of course can be traced in part to sensational media headlines following the release of research into the effects of chronic cannabis abuse. Yet the anti-drug lobby has been willingly involved in the perpetuation of self serving and frequently egregious falsehoods that have left inhumane policy sabotage and damaged individuals in their wake. Worse, the very real and well understood problems associated with cannabis abuse have been scattered by the gale of “cannabis psychosis”.
I should stress this is not a pro-drug nor pro-cannabis post. If anything it is a pro-evidence post and I would hope readers can reflect upon the value of evidence in a human rights manner, much as we do in a consumer rights manner. As I suggest under my “About” tab, skeptics make excellent agents of morality because they are agents of evidence. This isn’t to suggest one is endowed with superior morale. Rather, one is bound to reject subjective and predisposed constraints in favour of evidence.
An effective informed policy on cannabis use should not slant only toward the harms caused by its use but also by the harms caused by the social measures/existing policies designed to control or prevent its use. Cannabis is not a hard drug. Cannabis is not a soft drug. Cannabis is a drug, and as such deserves the respect that science and apolitical critiques can bring.
The nonsense above was originally written in 1988 and has been continually polished and rephrased over the years. Its most recent incarnation was Cannabis – suicide, schizophrenia and other ill effects, uproariously tagged “First Edition, March 2009”. Subtitled A research paper on the effects of acute and chronic cannabis use, it is in fact a biased selection of literature. Not research, nor literature review.
Cannabis “potency” is a key driver of fear and a launch pad for ongoing misinformation. This area is fraught with notable disrespect for variables involved. Is “potency” THC content per volume? If so, what strains grown under what conditions provide conclusive answers? Or does one compare the hashish and hash oil of the 1970s and 1980s (at around 20% THC content) with todays plants? If so, what of the famed sinsemilla grown for decades?
DFA choose to refute Australia’s peak illicit drug body, the ANCD, and their “Evidence-based answers to cannabis questions: a review of the literature” (2006), which concluded no significant increase in THC content had occurred. This was challenged by the unqualified lobbyists with a preposterous figure of 30% THC content from an apparent – and unsourced – 1993 Australian Bureau of Criminal Intelligence claim. Readers were to be very afraid as the equally preposterous and unsourced joint potency from the 1960s was 0.5%
Could this even be true?
In THC content of cannabis in Australia: evidence and implications, Wayne Hall and Wendy Swift reported in 1999:
The major obstacle to testing these claims is that the THC content of cannabis products has not been systematically tested by any Australian police force over the period in which average THC content has been claimed to have increased.
Well, no, it appears to be fiction.
So why are DFA misleading the public this way? A primary area of community confusion and angst is the poorly reported association between psychosis and cannabis. The most fallacious is the “puff-puff, go mad” claim. It terrifies parents and this fear can persist in the absence of evidence. I must stress that negative experiences associated with ingesting THC can certainly be exacerbated by ingesting a volume of cannabis that contains more THC than a user is accustomed to. I’m not attempting to refute this possibility. I would add however, that user titration gives control to the cannabis user over the amount ingested. In this light a number of claims pushed by DFA demand criticism.
Primary is that DFA claim that the introduction of hydroponic cannabis (itself a spin-off of prohibition’s failure) brings with it [page 11]:
…a well demonstrated dose-response relationship between cannabis and its related drug-induced psychosis, where the greater amount of cannabis consumed correlates to a higher degree of risk of psychosis any three to fourfold increase is absolutely critical in any assessment of cannabis harms. When it is further considered that changed usage patterns, whereby users smoke only the multiple potent heads of the cannabis plant… the ANCD paper’s approach to potency is of concern.
Again, as we shall see below, this is not backed by evidence. What is drug-induced psychosis in this context? Sure, hydroponic production has provided the equivalent of sinsemilla-type product to users. Yet DFA then go on to cite the ANCD paper which confirms a tripling of THC figures in the USA. Quite correctly there is no reason to suggest this hasn’t occurred here, yet as the paper notes:
…the majority of THC levels in studies of [USA] cannabis seizures have remained under 5%.
So the ANCD conclusion that no evidence exists for huge THC increases in recent decades is valid. If anything users have more of the THC rich component of the plant, and less of the THC poor component. Hydroponics ensures rapid maturation and more flowering (head). Per plant there is more THC rich matter. But that matter is not notably more THC potent.
I hate to excessively mull this over, so to speak, but once again prohibition has placed better drugs for the same price into the hands of Aussie kids.
Let’s consider DFA’s claim that, “users smoke only the multiple potent heads of the cannabis plant”. They are challenging figures from 1970 to 1997. Returning again to Hall and Swift 1999, we see on page 8:
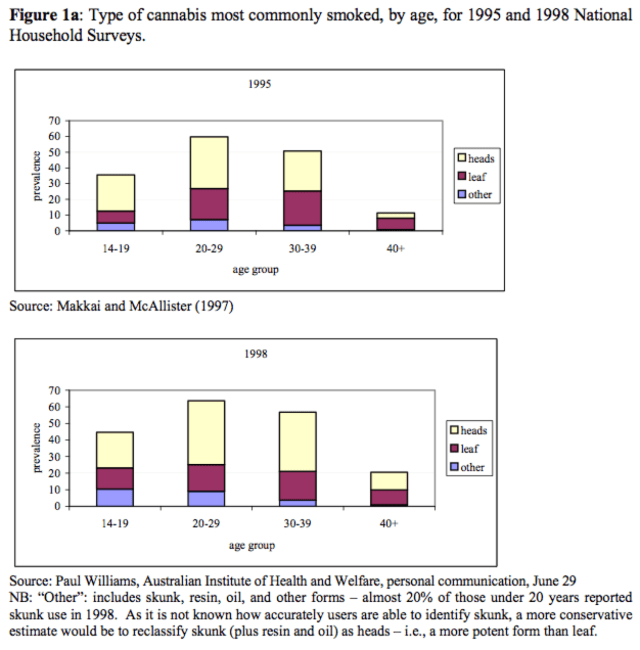
So consumption of “skunk” or “super-skunk” that DFA claim is driving kids insane increased as much as leaf in the 14-19 year old group, from 1995-1998. Yet head seems to be the main product. Nonetheless users are not “smoking only multiple potent heads”. Which sounds more scary than just “heads”, one presumes.
Under Changing Patterns of Cannabis Use, Hall and Swift write on page 7:
The media preoccupation with the THC content of cannabis has distracted attention from other causes for concern about changing patterns of cannabis use among Australian adolescents and young adults. These patterns of cannabis use, which may encourage younger users to use more potent forms of cannabis, may also increase their chances of developing problems as a consequence of their cannabis use.
This is of course, exactly the point. By pursuing sensationalism, co-morbid health problems and negative lifestyle changes are frequently ignored. That this has been willingly and eagerly encouraged by groups such as DFA as part of their agenda to encourage blanket illicit drug zero tolerance and the public health damage this brings, is deeply concerning.
In 2009 this manuscript of misinformation was used to lobby independent conservative QLD MP, Peter Wellington to push for the old DFA staple of School Drug Testing. Such tactics are typical of the evangelical crusade waged by this conservative Christian group. The Australian National Council on Drugs concluded in 2007 that SDT was technically unreliable, cost prohibitive, morally and legally problematic, prone to exacerbate problems faced by at-risk children, designed to normalise punitive measures and fraught with false positives.
You can read more here about Drug Free Australia and their campaign against evidence. Or just marvel at a school kid’s drawing of God espousing “be drug free and you’ll be with me”. It isn’t just punitive policies DFA seek but a quite inhumane roll back of Harm Minimisation strategies, particularly those involving harm reduction. Whilst it is unacceptable for young Aussies to be under the impression cannabis is entirely safe, we can see without much effort how a spike in reports on cannabis and psychological harm has been exploited.
Claims that cannabis is supposedly endowed with benign or even beneficial properties because it is “natural” are equally concerning. The notion that if something comes from the earth it’s therefore by default superior to a manufactured pharmaceutical analogue is certainly not backed by evidence.
In fact this point is ripe for confusion about the role of evidence, its import and what might be termed insults from intuitive reasoning. Cannabis use as a recreational drug is defended at times with argument from antiquity. Combined with the “mother earth” line it may sound quite compelling. Like many alternatives to medicine (such as TCM), cannabis is also subject to further defence with argument from antiquity. According to The Mayo Clinic medicinal use can be traced back 5,000 years. Yet a crucial distinction is made here.
Research into the medicinal benefit of cannabinoids or their application as medication is quite different from inhaling cannabis smoke and expecting better health. There is quite a lot of rot about cannabis being medicinally magical. Whilst there is some potential for a rather large range of symptoms and side effects, grasping impact on actual pathologies demands extensive investment in research.
As abundantly hinted at above, perhaps the most alarming and challenging theme I’ve faced in recent years is the media construct that cannabis “causes” psychosis or schizophrenia. The primary reason this created so much angst in the illicit drug policy and discourse deconstruction fields was the immediate negative impact on management of the many known psychological issues. The 2007 meta-analysis by Moore et al published in The Lancet was seized upon as conclusive evidence.
It remains an excellent review, and fortunately drew much needed explanation about the nature of meta-analyses and in particular that of Moore et al. Amidst the frustrating and very disappointing bad science reporting to follow (including one of the worst by Australia’s own Jonica Newby on ABC’s Catalyst), were calmer voices such as that found on Storied Conduct: Resources and News in Psychology.
Correlation, as our basic research theories tell us, can never prove causation. All of the studies examined by Moore et al. (2007) were correlational in nature. Further, the additional use of meta-analytic grouping techniques cannot turn correlational data into experimental data no matter how sophisticated the statistics. This means that, while the trends and the thrust of the data seems to make marijuana a very promising explanatory causal factor in the development of some of the psychoses that these research participants developed, such a link has not been conclusively demonstrated. And, while the gross odds ratio speaks of a 41% increased risk, the authors themselves acknowledge the impact of confounding and other variables in lowering the risk percentage in the studies they examined. Hence, we are left without a good estimate of what the actual increased risk might be.
The number of media articles poorly reporting findings grew steadily over three to four years. Diligently a steady number of D&A workers, bloggers and independent media contributors used a dual method of exposing predetermined agendas and explaining the results in proper context. Generically speaking – and I stress generically – the headline “Cannabis induced psychosis increases 300% in two years scientists find”, might pop up. On examination it reflects that a sample with 0.2% predisposition to psychotic episodes had two years later, under different methodology, been found to present a 0.6% prediction to experience the transient psychosis they are genetically predisposed to, had they continued to smoke cannabis heavily for another decade.
One of the sadder developments was the establishment in 2008 of the National Cannabis Prevention and Information Centre. The NCPIC. Coined the National Cannabis Propaganda and Infotainment Centre by a contributor to a professional e-list, it regretfully offers themes well documented as not being efficacious in reducing cannabis abuse. In 2009 NCPIC head Jan Copeland was pulled up by the same publication for dodging the need to publish bipartisan research.
The NCPIC is in the habit of presenting the style of faux science we see above from DFA and also using alarming distortion of facts in their supposed quest to “prevent”. The public is seemingly deemed at risk from balanced information which is substituted with bias and deception. In view of the documented harm this approach leads to it is not good enough for a tax payer funded organisation.
One of the best papers I’ve read is Continued cannabis use and the risk of incidence and persistence of psychotic symptoms: 10 year follow up cohort study, by Kuepper et al. This paper controlled very well for baseline incidence (Eg: self medication of psychosis/schizophrenia, supplementation of low cerebral anandamide [thus proposed alleviation of psychotic symptoms] via cannabis, cumulative effect of CBD’s anti-psychotic properties, other drugs, unstable lifestyle, etc.
In doing so, they thus also controlled for the host of suspected [exact cause remains unknown] causes of psychosis (stress, genetic predisposition, changes at puberty, assault, major life changes, biological causes, neuroses etc). This was itself arguably misused by Professor Jan Copeland who we’ve just met.
Wayne Hall and Louisa Degenhardt contributed an excellent review [BMJ 2011;342:d719] at the time. They noted the superior methodology and also that:
In the light of these findings and those of earlier studies, it is likely that cannabis use precipitates schizophrenia in people who are vulnerable because of a personal or family history of schizophrenia… A modelling study suggests that we would need to prevent 2018-4530 young people in the United Kingdom from becoming regular cannabis users to prevent one case of schizophrenia, or to prevent four to five times as many (10,000-23,000) from light cannabis use to achieve the same result.
Of course schizophrenia is a disease with a clear diagnosis. Psychosis is a transient symptom with a much less clear delineation. What’s certain is that the term is misused and frequently in the manner suggesting cannabis use/abuse leads to a permanent state of psychosis.
Copeland is quoted in an article for The Drum by Quentin Dempster:
Professor Jan Copeland, director of the NCPIC a government-backed preventative agency, told 7.30 NSW that if cannabis was taken out of the picture the incidence of schizophrenia in Australia could be reduced by 8 to 14 per cent. She could not be more specific. That guesstimate was based on overseas studies. There have been no studies in Australia. This is revealing.
I had seen the report and was stunned. Copeland had failed to grasp the import of incident cannabis use to incident psychotic symptoms. More so she had failed to appreciate the basics of the different time periods. What she had messed up re 8% and 14% from the Kuepper et al study came from this line in the Abstract under Results:
The incidence rate of [sub threshold] psychotic symptoms over the period from baseline to T2 was 31% (152) in exposed individuals versus 20% (284) in non-exposed individuals; over the period from T2 to T3 these rates were 14% (108) and 8% (49), respectively.
The paper cited mentions “schizophrenia” twice. Once in describing instruments used to collate data and again under “methodological issues”.
I wrote to Jan and rather comprehensively outlined the incident specific nature of the results, to seek clarification. I received no reply. For the record here is the conclusion from this sterling study.
Cannabis use is a risk factor for the development of incident psychotic symptoms. Continued cannabis use might increase the risk for psychotic disorder by impacting on the persistence of symptoms.
It’s important to realise that this association is emerging as a very small but very significant issue for individuals predisposed to psychotic episodes. “Cannabis induced psychosis” is thus better viewed as schizophrenia. To date new trends and good research has been seized or sabotaged for political gain. There are areas in need of research dollars wherein we should despise bad science or exploitation of good science. Illicit drug policy is one of them.
As I mentioned way above this is not a pro-cannabis post. There are a host of reasons including psychological, physical and social to not use cannabis. Although I note it is Australia’s most popular illicit drug.
Which reminds me. There are no reasons to not use and respect evidence.
