The Australian Skeptics National Convention is being held in Melbourne this year, at the University of Melbourne Parkville campus. Tickets are now on sale.
Early bird discount of 5% applies to convention tickets until 31 July 2023.
The convention will be held over Saturday 2nd and Sunday 3rd December at the Ian Potter auditorium, in the Kenneth Myer building (Google maps reference). Online access is also an option. To date, international speakers include critical thinker Melanie Trecek-King and well known skeptic activist Susan Gerbic. Keep an eye on the Skepticon 2023 website or check back here for updates, as the full speaker’s schedule continues to take shape.
Skepticon is known for presenting great speakers and stimulating topics. Recent conventions have included presentations on pseudo-archaeology, research into vaping, responding to the COVID pandemic, superstition in elite sporting performance, adaptation to climate change, the Ivermectin scandal, discerning trustworthy scientific studies and escaping cults. Speakers have included Dr. Ken Harvey, Dr. Rachael Dunlop, members of the European Skeptics podcast, Brian Dunning of Skeptoid, Steven Novella, Bruce Baer Arnold and great panel discussions, to offer just a hint of what this convention brings.
The annual Skepticon dinner will be held on the Saturday night at St. Andrews Hotel, Nicholson Street Fitzroy. It’s a popular night of entertainment, dining, great conversation and the presentation of awards from Australian Skeptics Inc. One is a unique prize that inevitably draws some media comment. Namely, The Bent Spoon Award.
This exclusive title is an annual award presented to the perpetrator of the most preposterous piece of paranormal or pseudo-scientific piffle. Nominations are underway for this year’s winner. Or should that be “lucky loser”? They include, but are not limited to favourites of this author, such as Dave Oneegs, Senator Gerard Rennick and (suspended) Dr. William Bay. If you have somebody in mind or want to add your support to an existing nomination, submit your vote by email.
Last years winner was bogus-medico Maria Carmela Pau who was caught out selling fake COVID vaccination exemption certificates. Other winners include Craig Kelly, 2021, for spreading his waffle on COVID, the vaccine, alternative “cures” and various conspiracy theories. Pete Evans, 2015 for dietary nonsense, anti-fluoride and anti-vaccination piffle. Pete also won in 2020, for his colourful but useless BioCharger, and yet more prolonged anti-vaccination rhetoric. What’s that? No, no. A haircut, no matter how preposterous, is neither paranormal nor pseudoscientific.
2016 was a great year, producing the winning trifecta of Judy Wilyman, Brian Martin and the University of Wollongong. This came in the wake of a doctorate being awarded for Wilyman’s anti-vaccine thesis, void of any research design or novel data. SBS-TV, ABC programmes and producers have also won for presenting pseudoscience and alternatives to medicine in a supportive framework. Of course dear reader I cannot omit that the 2009 Bent Spoon went to Meryl Wynn Dorey and the AVN for being themselves.
Justifiably, there are merit awards given for great talent and hard work. At a time when we are surrounded by conspiracy theories, scams, pseudoscientific claims, discrimination and bigotry, the skeptic movement is motivated to recognise and reward individuals who contribute to critical thinking, scientific reasoning and who value diversity and inclusivity. This is particularly clear in the Goals of Australian Skeptics Inc.
To this end, the following awards are also presented at the Skepticon Saturday dinner. The Fred Thornett Award – known as The Fred – is given for the promotion of, and educating the public about, issues of Science and Reason. The Barry Williams Award for Skeptical Journalism, also known as The Wallaby, acknowledges journalistic work that critically analyses or exposes issues related to pseudoscience or the paranormal. Depending on the topic, individuals chosen for these awards may have faced abuse and/or intimidation as they work toward these valuable goals. This is not lost on skeptics in Australia.
Finally, Skeptic of The Year is awarded to a skeptic or someone with links to the skeptical community in recognition of effective activism or an exceptional contribution to the skeptic movement. This is not awarded annually or biannually, but rather in response to an individual’s unique contribution.
Throughout the weekend there is opportunity for stimulating discussion with like-minded individuals on topical issues relevant to Skepticism. It’s also a great time to broaden your interest in, or involvement with, the skeptical community.
In a previous post we looked at the unsuccessful attempt of the Australian Vaccination-risks Network to convince the Federal Court of Australia it had legal standing to challenge the COVID-19 vaccine rollout.
They sought a writ of Mandamus to overturn provisional registration of mRNA and AstraZeneca COVID-19 vaccines, and a Judicial Review to overturn provisional approval of Pfizer’s vaccine for 5 to 11 year olds.
The evidence was intended to demonstrate lack of safety and efficacy of the vaccines. The plaintiffs contended the vaccines should not have been provisionally approved or registered. Indeed, that they should have been cancelled or suspended because of an imminent risk of death or serious injury. Thus, the Secretary of the Department of Health had erred in his duty to “cause to be maintained” the Australian Register of Therapeutic Goods.
However the evidence and legal arguments were never heard in court. The AVN had no “special interest”, and thus standing. On 8 August 2022 their appeal against this finding was found to be incompetent. A couple of months later, lengthy correspondence went out to all “donors and potential donors”. Headed AVN Legal Actions and Strategiesthe document opined on the issue of standing:
The way that the current case law is being applied by the Federal Court is essentially to say that nobody has sufficient standing to challenge these therapeutic ‘goods’, nor indeed the Secretary of Health.
The Babies Case
The AVN had decided to take “an alternative course of action”. One that had been researched and prepared by retired barrister Julian Gillespie and solicitors Peter Fam of Maat’s Method and Katie Ashby-Koppens of PJ O’Brien and Associates. In view of the AVN’s recent outcome it was deemed wiser to approach the High Court with “The Australian Babies Case” (AuBC), and seek to “halt the provisional approval of the Moderna jab from being injected into our precious 6 month old to 5 year old infants”. The AVN would “change course” and become a co-applicant with five others.
The other applicants were:
Associate Professor Peter Parry
Dr. Julian Fidge
Dr. Shoba Iyer
Dr. Astria Lefringhausen
Mark Neugebauer
The first three applicants above are active members of the Australian Medical Professionals’ Society (AMPS), a Red Union group that formed with the specific aim of challenging the rollout of COVID-19 vaccines, fighting COVID-19 mandates and promoting controversial treatments such as Ivermectin and hydroxychloroquine. Parry is also the lead applicant challenging the State of QLD over health professional’s vaccine requirements and a key member of Doctors Against Mandates. Three months before the AuBC strategy was outlined in this document, the AVN published the full AMPS Medico-Legal Summit on its website.
The breakdown of speakers at the summit includes AVN legal consultant and primary researcher behind the AuBC Julian Gillespie, primary plaintiff Prof. Peter Parry, Senator Malcolm Roberts and Senator Gerard Rennick. We will meet Senator Rennick again, later in this post. In lobbying the SA Minister for Child Protection, plaintiff Mark Neugebauer cites AMPS correspondence from Dr. Christopher Neil, another speaker at the summit. Gillespie and Ashby-Koppens appear on AMPS Discussions From The Frontlineupdating legal activity |2|.
The document went on to outline the strategy behind this new approach:
In The Australian Babies Case, the legal strategy is to present five applicants before the High Court of Australia, and show the Court how each applicant is affected by the actions and inactions of the Secretary of Health, with respect to the Covid-19 drugs made available to babies and young children, and the rest of the Australian community in circumstances where, prima facie, preventable deaths, illnesses, and injuries in extraordinary numbers are associated with their use; and where most of the population does not need them; however despite the expertise and evidence possessed by the various five applicants, the current law on standing in Australia is deficient, and will not recognise any of the applicants as proper parties for suing the Secretary of Health.
Australian Babies Case legal research team
Julian GillespiePeter FamKatie Ashby-Koppens
It further outlined that the Babies Case would be seeking to have the High Court “fix the law on standing” such that the applicants would be accepted as having “special interest”. Namely, “the preservation of human life from preventable death, illness or injury”. It was claimed, albeit without evidence, these preventable outcomes were being seen now, due to “COVID-19 drugs” and that this constituted an “iatrogenic catastrophe”. That is to say, a catastrophe caused by the diagnosis and treatment of a condition.
Mark Robinson SC who represented the AVN in the initial failed case, confirmed this new approach was viable and advised that the High Court “has indicated that it wishes to revisit the law of standing in Australia”. They would be seeking:
A new Special Interest regarding the preservation of human life.
If successful, a court-granted injunction to halt the provisional approval of COVID-19 vaccines to babies 6 months to 5 years and children 6 to 11 years of age.
If the High court recognises this new special interest for standing, that the High or Federal Court immediately hear the Judicial Review cases for both childhood age groups and the original Mandamus case for mRNA and AstraZeneca vaccines.
If successful, the AVN expected to be able to proceed with their initial cases. As “a matter of convenience” the AVN would seek to take over the running of the Judicial Review case that involved children 6 months to 5 years (the AuBC). The AVN note that they feel joining the case “operates as a de facto appeal” from the 8 August 2022 Federal Court appeal decision.
The application was filed with the High Court on 20 December 2022. The day before, a media release was published by AVN president Meryl Dorey. It provided some initial insight into the legal tactics to be employed in this quest for a new category of standing. Resurrected anti-vaccine themes from the initial Federal Court case peppered a quote attributed to Julian Gillespie (bold mine):
The High Court of Australia is now being called upon to protect our youngest from participating in an acknowledged and ongoing Phase III clinical trial, to receive experimental drugs involving unprecedented levels of reported adverse events, including deaths… for a virus also acknowledged to pose no threat to our Babies and Toddlers…
At this point it’s worth noting that, in public discourse, the Australian Babies Case legal team studiously avoid discussing the 3 August 2022 ATAGI recommendations for this age group. Namely:
ATAGI recommends COVID-19 vaccination for children aged 6 months to <5 years with severe immunocompromise, disability, and those who have complex and/or multiple health conditions which increase the risk of severe COVID-19.
More so, the legal team make much of the fact severe cases of COVID-19 are not common in this age group, and thus provisional approval of Spikevax suggests nefarious, and not clinical, motivation. Yet ATAGI clearly state:
ATAGI’s guidance takes into account:
The very low risk of severe COVID-19 (e.g. hospitalisation due to COVID-19) in healthy children aged 6 months to <5 years. This age group is one of the least likely age groups to require hospitalisation due to COVID-19. Among the small number who are hospitalised or who die due to COVID-19, underlying medical conditions or immunocompromise are frequently present. […]
The plaintiffs alleged Spikevax is a “genetically modified organism”. As such, Brendan Murphy, Secretary of the Department of Health had failed to comply with yet another section of the Therapeutic Goods Act 1989 (TG Act). As expected a writ of certiorari would be sought to quash provisional approval of Moderna’s Spikevax vaccine for children 6 months to 5 years. A writ of mandamus (where the court orders an official) was originally sought to have the application to approve Spikevax, reviewed under law. It was ultimately abandoned. For more specific insight we must turn to the application.
Legal Arguments
The plaintiff’s argument had two grounds, and a section headed Reasons Why Remittal Not Appropriate. Those reasons argued that the case should be heard by the High Court because that court had the power to accept the need for, and then admit for hearing, a new category of standing. Thus the High Court should not remit (send back) the case to the Federal Court. They contended that the principles for standing should be more liberal when a person can establish the subject matter involves life threatening or debilitating medical conditions and they seek to preserve human life. In short:
Where the fabric of human life might be compromised or adversely impacted, interested and involved members of the public should have a right of standing in such circumstances.
Whilst I don’t accept the argument for a new category of standing in this manner, I do agree that the law is frequently lacking. In fact, it’s about here I suspect a number of Australian vaccine proponents, Skeptics and opponents of the anti-vaccination lobby may feel a dash of Deja Vu.
In 2010, following complaints from the public about misleading AVN advice, the NSW Health Care Complaints Commission published a “damning report”. The AVN successfully appealed the ruling because whilst the HCCC had jurisdiction, the complaints lacked evidence that anyone had acted on AVN advice. The appeal outcome led to the Health Legislation Amendment Bill 2013 in NSW Parliament, allowing the HCCC to act on the likelihood of harm. A follow up inquiry was launched and a second, more in depth Public Warning against the AVN was published in 2014.
Let’s return to the present. The plaintiffs also argue that there are “important questions about the lawfulness of Commonwealth officials to make provisional determinations” that impact wellbeing. They allege there is no real jurisprudence about this in the context of the TG Act. Yet in reality, the standard of evidence required to make these determinations is high and the TG Act is comprehensively designed to minimise risk. Indeed failure to make provisional determinations may risk the wellbeing of the nation.
Ground One of the plaintiff’s argument again takes us to the TG Act. Specifically Section 22D(1), which provides that the Secretary must decide to make or refuse to make a determination, when a valid application has been made. In this case the application was for Spikevax (elasomeran), which the Secretary provisionally approved for children 6 months to 5 years, on 19 July 2022. The plaintiffs argue that s 22D(1) “is subject to an implied restraint”, that the decision will be legally reasonable. They submitted:
Legal reasonableness, or an absence of legal unreasonableness, is an essential element in the lawfulness of decision-making.
Referring to “the decision” to provisionally approve Spikevax for the ages under discussion, the application is dismissive of evidence used. It cites the TGA document Australian Public Assessment Report for Spikevax, 19 July 2022. Yet the Submission overview and risk/benefit assessment, accommodates no less than half of the 31 pages. This was updated on 8 November 2022; 42 days prior to filing of the plaintiff’s application, and contains 8 subsections covering 55 of the document’s 69 pages. Subsections include, but are not limited to, Quality, Risk management plan, Risk-benefit analysis, Additional clinical data and Second risk-benefit analysis.
The plaintiffs further argued that the Secretary’s decision that Regulation 10L(1)(a) of the Therapeutic Goods Regulations 1990 (TG Regs) was met, is legally unreasonable. That particular regulation states under Provisional Determinations:
(1) For the purposes of subsection 22D(2) of the Act, the criteria are all of the following:
(a) an indication of the medicine is the treatment, prevention or diagnosis of a life-threatening or seriously debilitating condition;
In other words it was legally unreasonable to accept that the vaccine ever contributed to the prevention of serious illness brought on by COVID-19 in children 6 months to 5 years. This argument is a repeat of the AVN tactic seeking Judicial Review in the initial Federal Court Children Decision case, where they also targeted s 22D of the Act.
This was cited because the AVN also sought an order quashing any determination made by the Secretary pursuant to section 22D, that an indication of the vaccine:
“[W]as the treatment, prevention or diagnosis of a life-threatening or seriously debilitating condition for children aged 5 to 11 years of age.”
The plaintiffs continue to argue their case for “legal unreasonable decision-making” by again turning to the TG Act. They argue the Secretary has failed to satisfy requirements in s 25(1)(d)(i). Section 25 deals with evaluation of therapeutic goods, and the cited subsection provides:
(d) for an application for provisional registration of a medicine:
(i) whether, based on preliminary clinical data, the safety and efficacy of the medicine for the purposes for which it is to be used have been satisfactorily established.
Put more simply, the plaintiffs contend that when the Secretary was evaluating Spikevax, the data he used did not “satisfactorily establish” its safety and efficacy. This, they allege, amounts to legal unreasonable decision-making.
Genetically Modified Organism
Ground two of the plaintiff’s argument stated that the Secretary failed to comply with s 30C(2) of the TG Act. Section 30C provides for Consultation with the Gene Technology Regulator (OGTR). The cited subsection reads:
It appears that there has been non-compliance with a statutory condition in the TG Act. […] The plaintiffs contend that non-compliance with the statutory obligation mandated by s 30C(2) leads to the invalidity of the registration decision that followed.
Could it be that the Secretary did not have to notify the OGTR? As fate would have it we are assisted here by questions from Senator Gerard Rennick. On 16 February 2023 during a Community Affairs Legislation Committee Estimates hearing, Rennick questioned our current gene technology regulator, Dr. Raj Bhula, about s 30C of the TG Act, asking if the Secretary had written to the OGTR in regards to mRNA vaccines.
You can read the full exchange on Rennick’s website, or watch the video of it below. However, I’ll cut to the responses that matter with respect to the AuBC. Does the Secretary have to notify the OGTR?
Dr Bhula : No, because the mRNA vaccines are not required to be regulated through the OGTR.
Senator RENNICK: Did they write to you and actually ask you that question?
Dr Bhula : No, because they’re not required to be regulated through the OGTR.
Senator RENNICK: But how would they know, because you’re the expert? And, by the way, gene technology involves both replication and transcription.
Dr Bhula : Yes.
Senator RENNICK: Which is what the mRNA vaccine does.
Dr Bhula : But the mRNA COVID-19 vaccines did not involve any step of genetic modification—
Senator RENNICK: They produce proteins.
Dr Bhula : or a GMO—
CHAIR: Senator Rennick, would you allow Dr Bhula to finish her answers.
Dr Bhula : which meant that that didn’t require regulatory oversight by the OGTR.
An unambiguous answer. Interestingly, this wasn’t published on Rennick’s website at the time of the exchange. It was published 20 March 2023, which was four days after the High Court decided not to hear the AuBC. A coincidence? Unlikely, dear reader. As mentioned above, Senator Rennick, the AuBC plaintiffs, key legal researcher for the case and the AMPS are linked by their COVID-19 ideology and related lobbyist activity.
Gerard Rennick questions Dr. Raj Bhula, Office of Gene Technology Regulator
For the purposes of the AuBC affidavit, I acknowledge the confusion surrounding mRNA vaccines and GM technology. The AstraZeneca COVID-19 vaccine using a genetically modified chimpanzee adenovirus, is a clear example of GM technology. The OGTR Risk Assessment and Risk Management Plan for that vaccine is here. Years earlier the OGTR published a similar plan for a GM Live Attenuated Influenza Vaccine. The TGA acknowledges both examples as GMO medicines.
Technology applied to extract, multiply and distill the mRNA used in vaccines to instruct our cells to produce the spike protein of SARS-CoV-2 is different to the genetic modification of an adenovirus or a live influenza virus. Dr. Bhula describes it as not involving “any step of genetic modification or a GMO”.
Nonetheless, the Australian National Gene Technology Scheme lists mRNA COVID-19 vaccines, including Spikevax, as GMOs used as medicines. An Open Access Government article states, “mRNA and viral vector vaccines are derived using techniques of genetic modification (GM)”. The Alliance For Science distinguishes between the two. “This one really is genetically engineered”, it says of the adenovirus vaccine, after discussing mRNA vaccines.
We must accept Dr. Bhula’s position that mRNA vaccines are not required to be regulated through the OGTR. For the sake of the AuBC affidavit, s 30C(2) of the TG Act does not then apply, and the provisional registration of the mRNA vaccine Spikevax, is valid.
Case Remitted to Federal Court
The plaintiffs did not appear before the High Court. On 16 March 2023, Justice Stephen Gageler remitted the case to the Federal Court of NSW, as per the following order. A summary page is below.
No weight was given to the legal arguments raised, although it was noted there were “supporting affidavits totalling more than 2,000 pages”. What’s important is Justice Gageler’s observation that the Secretary had submitted that the proceedings should be remitted to the Federal Court which would have jurisdiction, under Section 39B(1) or (1A)(c) of the Judiciary Act. That section follows parliamentary action in 1997, to transform the Federal Court into one with more general jurisdiction (see p.9), including jurisdiction over any matter, “arising under any laws made by the Parliament [excluding criminal implications]”.
Justice Gageler observed:
I am satisfied that this matter is one “arising under” the TG Act for purposes of s 39B(1A)(c) of the Judiciary Act, and that the Federal Court has jurisdiction over its subject-matter and the parties on that basis.
Justice Gageler reflected on the plaintiff’s claim that the High Court was the only appropriate Court to decide on a new category of standing due to “special interest” arising when “the fabric of human life might be compromised or adversely impacted”. He stressed that the power to remit is discretionary “to be exercised after due consideration of all the circumstances of the case”. Justice Gageler cited another case as instructive, in that the power of the remitter is designed to ensure the High Court is not diverted from its principle functions by matters that “could properly be brought in an Australian trial court”. After offering his assessment of the significant scale of the case, Gageler concludes:
Having regard to these considerations, significant case management and fact finding are likely to be required to conduct a hearing of the kind contemplated by the application. Undertaking that task would unduly divert the Court from its principal functions.
“We are Discontinuing the Australian Babies Case”
The plaintiffs did not return to the Federal Court. On 12 April 2023, instructing solicitor Peter Fam of Maat’s Method published an article, and a longer explanatory video, in which he labels the vaccines “a poison”. In view of their 2022 failures with the Federal Court, further chances were poor. Even if successful, there may be repeated appeals lasting over a year. They did not have the money or time. “People are being injured and dying every day”, from COVID-19 vaccines, Fam said without evidence.
Fam added; “Too much money has been usedon facetious exploits and actions… things that haven’t been thought out in terms of strategy… people aren’t working together… doing things that are contradictory to each other… I have to take some responsibility… we lost the AVN case… a lot of money had been donated to that case”.
However:
All is not lost. This is a pivot; not a retreat, and there are other matters we have been working on simultaneously with this one, with better prospects of success than this case would have in the Federal Court. Those efforts will be formally launched within weeks, and you will hear more about them soon.
Dr. William Bay
A final mention must go to suspended GP registrar, William Bay. Bay has become a favourite amongst “cooker” watchers since he chose an AMA conference to film himself yelling anti-vaccine conspiracies, and call Chief Medical Officer, Paul Kelly “a liar”. A client of Peter Fam, Bay was asked to join the AuBC as a plaintiff. Shortly after he wanted to swap his position as plaintiff with the parent of a vaccine-injured child, believing this gave the team a greater chance at success. Fam and Gillespie disagreed. Nor could such a client be found.
Later, he filed for leave to intervene in the case as he objected to the nature of the special interest standing. He argued that if granted, the existence of standing granted via special interest in “the preservation of human life from preventable death, illness or injury”, could be used to justify COVID-19 vaccination for children. You can read Julian Gillespie’s “urgent” letter to supporters on this matter here.
Understandably, Bay further argues that such special interest standing may then be used to interfere in the application of medicine and the doctor-patient relationship in areas unrelated to COVID-19 vaccination (see video 56:45). Gillespie argues, quite rightly, that the request for standing applies to administrative and not private law. What Gillespie omits though, is any appreciation of how administrative changes impact private citizens.
Conclusion
The Australian Babies Case sought to convince the High Court to accept that medically qualified applicants had “special interest” preventing “death, illness or injury”, in babies and small children. Success would lead to a new category of standing, and this would permit the AVN to return to the Federal Court to pursue this case and its original 2022 Federal Court case, AVN v Secretary, Dept. Health.
Case evidence involved a revamping of prior legal tactics. The Therapeutic Goods Act was exploited by the plaintiffs to demonstrate regulatory failures on the part of the Secretary of the Department of Health. These failures, they again argue, justify overturning the registration or approval of COVID-19 vaccines. Driving this action was a suite of fallacious claims and misrepresented statistics.
The plaintiffs are members of and/or closely associated with the AMPS, a well organised union of medical and allied health professionals, working actively to undermine confidence in COVID-19 vaccines. Members of the legal team in this case are strident anti-vaccine activists, closely associated with AMPS, and outspoken anti-vaccine politicians.
Despite the label of “Babies Case”, this was all about giving the AVN a second chance for legal standing to have their case demanding an end to all COVID vaccines, heard in the Federal Court. Had standing been granted via a special interest as described above, it could be used to target all vaccines and help Meryl Dorey advance her life-long claim that “no vaccine is safe”.
According to the instructing solicitor of the AVN, further action should be expected soon.
During the second and third years of the COVID pandemic, skeptics began to hear more and more of an anti-parasitic drug that had been used frequently for animals and less so for humans.
Ivermectin has been approved by health authorities to treat humans with strongyloidiasis and onchocerciasis (river blindness): conditions that are caused by parasitic worms. Also there are topical ivermectin preparations used to manage skin conditions such as rosacea and external parasites such as head lice. Used as prescribed it is quite safe and has improved the lives of countless individuals in developing nations. Yet we weren’t hearing about ivermectin used in this manner. Thanks to disinformation and irresponsible repetition of dubious claims, ivermectin was being promoted as a means to combat COVID-19.
The anti-vaccination movement embraced ivermectin because it resonated with the “my body, my choice” mantra. Right leaning media identities promoted it in much the same illogical way as they had hydroxychloroquine. It had been used safely for decades, they argued, and thus was clearly a sound choice to combat COVID-19 symptoms. Yet hydroxychloroquine, had a pharmaceutical history as an anti-malarial and an agent to manage symptoms of arthritis and autoimmune disease, not in treating COVID-19. Ivermectin similarly, had no clinically proven background in the treatment of COVID-19. The clinical trials had simply not been done.
For skeptics, the issue was and is quite simple. Look toward reputable sources. Seriously examine the arguments in favour of ivermectin. Review the strength of research being cited. Place the issue in context. Keep an eye out for ideology. Check the profiles and backgrounds of key players, and so on. In short: Seek the evidence.
Initially there was the 3 April 2020 media release from Monash University. The Monash Biomedicine Discovery Institute announced a paper published in the peer reviewed journal Antiviral Research. The title, The FDA-approved drug ivermectin inhibits the replication of SARS-CoV-2 in vitro, was tantalising. An informative piece published in the Sydney Morning Herald on 22 October 2021 cites experienced drug developer Dr. Craig Rayner referring to the impact of the announcement:
“It was incredibly hyped,” Dr Rayner said. “I knew it was going to start a fire.” […]
“It’s not the best thing for Australia to become known for in terms of its contribution to the pandemic,” Dr Rayner said. “But that’s what it is, unfortunately. It has promoted vaccine hesitancy and people are dying because they’re taking a veterinary medicine that has not been proven.”
For those looking to grab the ivermectin ball and run with it, the media release was peppered with big names, other nasty diseases and potentially exciting findings. It has since been modified to include an FDA warning and offer clear disclaimers about ivermectin’s effectiveness. What mattered to those who would go on to push ivermectin as a safe cure for COVID-19, came from just a few paragraphs:
A collaborative study led by the Monash Biomedicine Discovery Institute (BDI) with the Peter Doherty Institute of Infection and Immunity (Doherty Institute), a joint venture of the University of Melbourne and Royal Melbourne Hospital, has shown that an anti-parasitic drug already available around the world kills the virus within 48 hours.
The Monash Biomedicine Discovery Institute’s Dr Kylie Wagstaff, who led the study, said the scientists showed that the drug, Ivermectin, stopped the SARS-CoV-2 virus growing in cell culture within 48 hours.
“We found that even a single dose could essentially remove all viral RNA by 48 hours and that even at 24 hours there was a really significant reduction in it,” Dr Wagstaff said.
Ivermectin is an FDA-approved anti-parasitic drug that has also been shown to be effective in vitro against a broad range of viruses including HIV, Dengue, Influenza and Zika virus.
Dr Wagstaff cautioned that the tests conducted in the study were in vitro and that trials needed to be carried out in people.
For those of us even broadly familiar with how drugs are brought to market, it was that final line above that mattered. Early lab results do not equate to clinical trials. Indeed shortly after the announcement, effort and funding across the globe was directed to clinical trials of ivermectin. Yet it would take almost eighteen months before enough studies were done, presenting enough evidence to show that ivermectin does not hold promise as a treatment for COVID-19. Over 2021, the number of news articles heavily critical of the “dubious” apparent “miracle cure” rose steadily such as here, here and here. The BBC published a powerful article on the “false science” backing ivermectin. Flawed data, fake evidence and poorly designed and written research was common.
Australia watched on as Malcolm Roberts, George Christensen, Craig Kelly and Clive Palmer promoted (and still promote) ivermectin. In the absence of evidence ivermectin could not be prescribed for COVID-19. This led to proponents sourcing and ingesting veterinary-grade ivermectin. It soon became clear from social media that many were taking excessive doses very often. On 21 August 2021 the FDA tweeted, “You are not a horse. You are not a cow. Seriously, y’all. Stop it.” That tweet links to accurate FDA information on the dangers of using ivermectin.
Since the inception of VAERS, anti-vaccination activists have misused reports as a cornerstone in their campaign to misinform and mislead. Vaccination against COVID-19 has led to that misuse exploding.
What is VAERS?
VAERS is the U.S. based Vaccine Adverse Event Reporting System managed by the Department of Health and Human Services (HHS) and co-managed by the Centers for Disease Control (CDC). It is an early warning system that collates reports of suspected adverse events following immunisation. A full explanation is here. Reports may be submitted by anyone who has received a vaccine authorised in the United States. Doctors, health workers, family members and associates can also submit reports. It is an open passive reporting system that allows reports from anyone who is aware of an adverse event they perceive as related to a vaccine.
It follows that the reports are just that; reports. Reports that contain no information about causality or indeed accuracy. This is not to say they are inaccurate. Rather that their true meaning, and indeed impact, can only be borne out in the context of further evaluation. Evaluation will assess any pattern of events, related health problems, any identifiable mechanism of causality and the time frame between vaccination and adverse event. Suspect vaccines would be suspended and emergency investigations employed to assess the scale and seriousness of adverse reaction(s). If the adverse event is confirmed to be more significant than in pre-licencing trials, the vaccine is removed from market.
Research and peer reviewed publication would follow, describing these findings. This information is of enormous benefit to the design, manufacture and trial of future vaccines. What stands out immediately is that determining adverse events due to vaccination requires significant input seperate from VAERS. The most important and irrefutable element about VAERS reports is that they do not represent cause and effect.
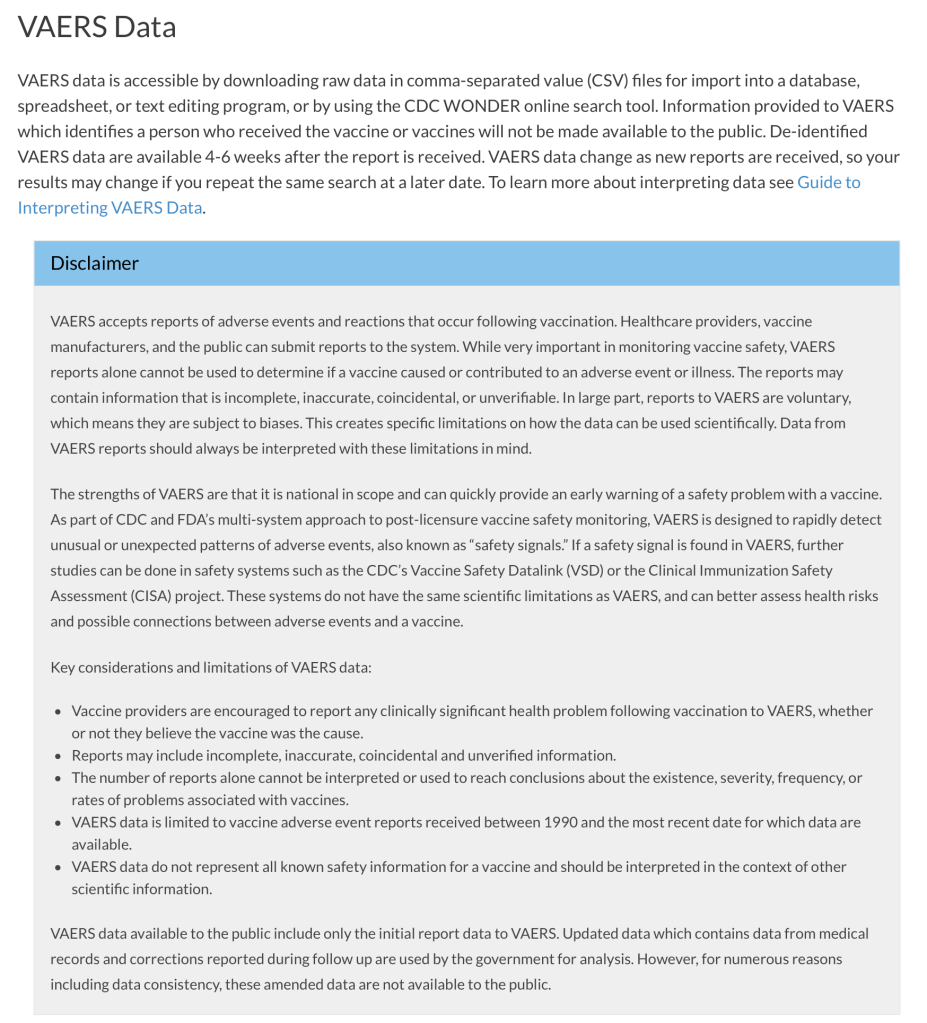
When evaluating data from VAERS, it is important to note that for any reported event, no cause-and-effect relationship has been established. […]
VAERS collects data on any adverse event following vaccination, be it coincidental or truly caused by a vaccine. The report of an adverse event to VAERS is not documentation that a vaccine caused the event.
Under VAERS Data Limitations:
Reports vary in quality and completeness. They often lack details and sometimes can have information that contains errors. […]
No proof that the event was caused by the vaccine is required in order for VAERS to accept the report. VAERS accepts all reports without judging whether the event was caused by the vaccine.
The above is a small selection from the guide. Yet it is enough to inform readers seeking definitive information on adverse events linked to vaccines, that it will not be found there. Exploiting the reports to provide an accurate picture of potential or existing problems takes resources. Resources that individuals don’t have. Consider the case of RotaShield. This rotavirus vaccine was taken off the U.S. market in 1999 because of an association between the vaccine and intussusception. The U.S. Advisory Committee on Immunisation Practices (ACIP) voted for its removal after an in depth review of available data. RotaShield was available for just months.
Paul Offit is well schooled in how VAERS is misused. He is also a firm supporter of civilian reporting because, as intended, unanticipated side effects can be caught this way. He has referred to VAERS as a “hypothesis-generating mechanism”, and observed about RotaShield:
There were a number of VAERS reports that patients within a week developed an intestinal blockage. A study was done and it was shown to be a causal association. VAERS was the tipoff. There’s value in it.
The suspected association between RRV-TV and intussusception based on a review of VAERS data led CDC, in conjunction with state and local health departments, to implement a case-control study [in 19 U.S. states among 429 infants and 1,763 matched controls] and case-series analysis and a retrospective cohort study [among 463,277 children].
So yes. If it’s confirmation of adverse events due to vaccination one seeks, merely perusing VAERS isn’t enough. This doesn’t stop antivaxxers from abusing the VAERS database to create the illusion of wide scale “vaccine injury”. As we’ve seen time and again during the COVID-19 vaccine rollout, screenshots and memes reach a large audience. Discredited Australian Instagram influencer and anti-vaccine advocate, Taylor Winterstein, has misused VAERS data to attack “mainstream mentality”. These tactics have the added advantage of side-stepping the guide to interpreting what is limited data on VAERS. The same approach is used by right wing cable news outlets. There are numerous techniques used to avoid the reality that there is only a temporal, and not a causal, relationship between vaccine and adverse reaction. Presenting government data carries a certain authority. Stripping it of context ensures it is inaccurate.
OpenVAERS
Post hoc ergo propter hoc: After this therefore because of this. This fallacy is the fuel driving the VAERS misinformation empire. Without it, outright claims cannot stand. Nor could the inference and extrapolation that comes from accepting widespread vaccine injury and death. The Vaxxed II bus in Australia is a typical example. It began last year, collecting dubious testimonials on “the vaccine-killed and injured”. Last month it began targeting the COVID-19 vaccine. Removing context from VAERS data ensures post hoc fallacy. This is exactly what the OpenVAERS project does. Launched in September 2019, it was initially run from archivist.net as confirmed on the Facebook page of The Archivist. In January 2021 the domain switched to openvaers.com and focused on COVID-19 vaccination data. Unsurprisingly OpenVAERS is a favourite of antivaxxers. Until recently, the index page offered:
The OpenVAERS Project allows browsing and searching of the reports without the need to compose an advanced search (more advanced searches can be done at medalerts.org or vaers.hhs.gov).
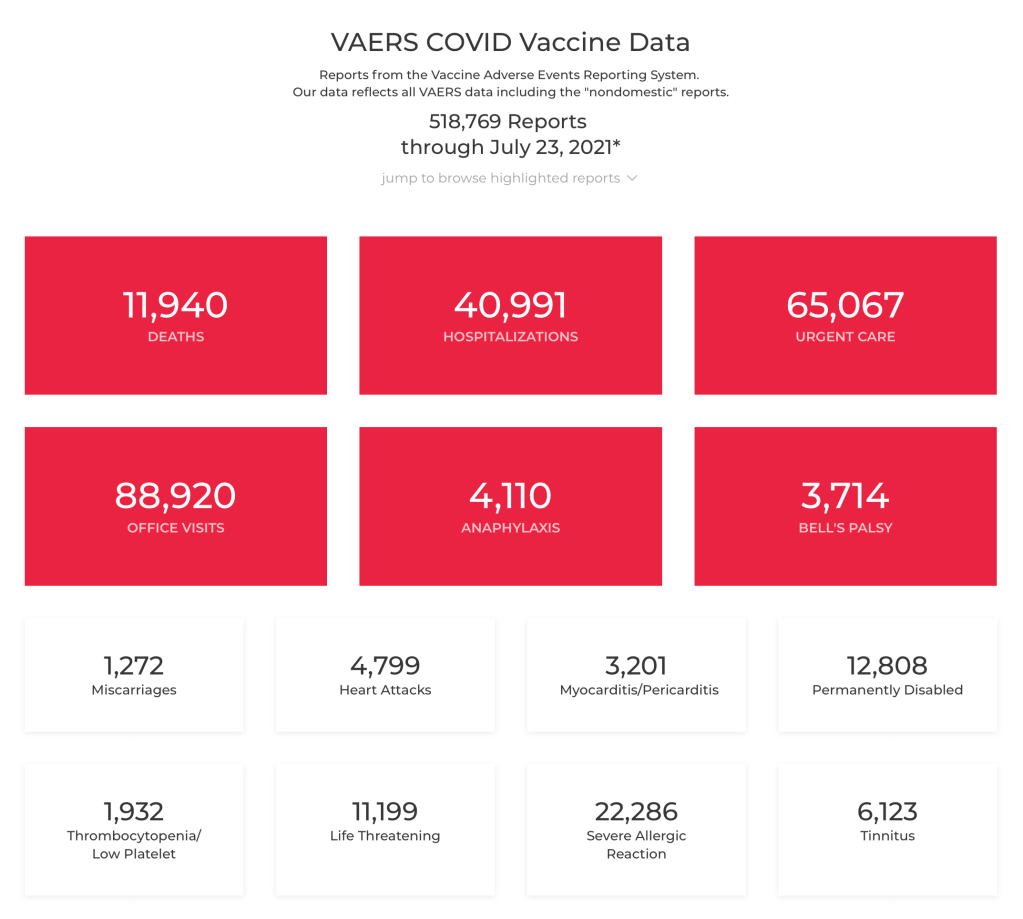
That’s what we find on the archived index page as at 1 August 2021. The next capture is 23 August 2021. At some time between these captures, OpenVAERS included a link to its own copy of the VAERS disclaimer both on the index page and its impactful VAERS COVID Vaccine Data page. The change on the vaccine data page was minor. Compare the 23 July and 20 August pages below. Keep in mind this is what readers see when they land on the data page. To appreciate the importance of context I’ve included a screenshot of the government VAERS data page.
Prior to this, users of OpenVAERS would have to navigate to the About page and follow the link to the VAERS About page. The change came just prior to the publication by Logically, a misinformation tracking group, of an article on 12 August which revealed the name and face behind the site. Logically had posed questions and a request for comment, which may have prompted the design change. Lizabeth Pearl Willner (below) better known as Liz Willner believes her daughter was injured by vaccination and began posting anti-vaccine content on social media in April 2019. She insists the site exists to provide easy access to official data.
There were significantly more visits to OpenVAERS (1.23 million) than to VAERS (796.63k) between February and July this year. Logically discovered that 30 percent of referrals to OpenVAERS are from the right wing, fake news site, Gateway Pundit. 10 percent are from conspiracy theorist Vernon Coleman (old man in a chair). These sites promote COVID conspiracies, pseudoscience and anti-vaccination rhetoric. Willner’s now deleted Facebook account and recently deactivated Twitter handle @1pissedoffmom1, amplified the reach and impact of OpenVAERS.
Until April 2021 OpenVAERS included a dedicated and searchable vaccine excipients table. The OpenVAERS blog now returns a 404 page. Indeed those behind OpenVAERS seem intent on having their deleted content also removed from archive.org. When running, the blog provided a one stop antivax shop for COVID-19 misinformation for “warrior moms, dads and grandparents”.
Call For Action posts contained alarming inaccuracies about the COVID-19 pandemic and the safety of the COVID-19 vaccine. The posts linked to ready-made PDFs to be printed out and mailed to “friends, family, and elected officials”. The drill, as they called it, was “10 copies, 10 stamps, 10 envelopes, 10 chances to wake someone up”.
Unfortunately, coronavirus vaccines excel at producing iatrogenic injury. Since their rushed introduction in December, these shots have produced four times more fatalities than the terrorist attacks on 9/11.
A link to that particular post, along with the 9/11 reference was shared onThe Defender. That’s the “news and views” site of Robert F. Kennedy Jr.’s Children’s Health Defense. The potential for harm by encouraging vaccine hesitancy in the midst of a pandemic is significant. Willner has ignored requests for comment from VICE News. The OpenVAERS blog also claims to be getting around “the criminal censorship of essential vaccine information on social media”.
Successful misuse of data this way relies upon the base rate fallacy. When vast sections of the population are involved, background mortality and morbidity become significant. Adverse events and deaths are reported in such numbers not because the vaccine is responsible, but because so many people are being vaccinated on any given day. Each person is given literature on how to report adverse reactions to VAERS. The V-Safe initiative includes regular text messages asking about any symptoms or changes to health. Attention given COVID-19 vaccination is unparalleled and this is reflected in data. Reports to VAERS (CSV VAERS Data accessed 3 September 2021) for all of 2020 totalled 63,544. To date, reports for 2021 ending 20 August, total 674,382. Not only are these reports unconfirmed but the safety of the COVID-19 vaccine is regularly affirmed.
Kolina Koltai is a Postdoctoral Fellow at the Center for an Informed Public based at the University of Washington. She describes OpenVAERS as “misinformation 101” and stresses that such decontextualisation is common to misinformation. Koltai uses such examples in classes that she teaches. In responses to questions posed by Logically, Liz Willner accused them of misrepresenting both VAERS and OpenVAERS. She cited data collected between 1990 – 2010 to argue, misleadingly, that “83% of reports are health care workers and Pharma”. Despite all evidence pointing to her, she insists OpenVAERS is a team effort. This is reflected on the site.
We built openVAERS because we found the HHS site difficult to navigate and get information from. We wanted a way to browse reports. Once we had that we decided to make it public.
How generous. Who is behind OpenVAERS?
OpenVAERS is a project developed by a small team of people with vaccine injuries or have children with vaccine injuries. We do not accept donations or solicit fees. There is zero monetization of this site. It is purely created in order to help others browse the VAERS records and to identify the reported signals that may otherwise get missed.
Here Willner misuses the term “signals”, specifically in how they relate to establishing risk. According to the CDC underHow VAERS works:
Patterns of adverse events, or an unusually high number of adverse events reported after a particular vaccine, are called “signals.” If a signal is identified through VAERS, scientists may conduct further studies to find out if the signal represents an actual risk.
The design of OpenVAERS allows immediate access to VAERS reports. These, in conjunction with tabulated figures, can be easily screenshot and spread via social media. Misleading commentary on these platforms aims to encourage vaccine hesitancy. One claim is that COVID-19 vaccines cause serious cardiac events and heart attack. In addressing this topic the indefatigable Orac picks apart flawed manipulation of data from Robert F. Kennedy Jr. and Children’s Health Defense. Back in May the energetic David Gorski addressed the “vaccine holocaust” based on VAERS data that Mike Adams bravely announced. Examples abound. The one constant, and undoubtedly something to be factored into public education, is that misuse of unverified reports is a key driver of vaccine hesitancy.
Despite long standing problems, VAERS works. RotaShield is a case in point. Twenty years of research preceded its approval by the FDA. Four months after ACIP recommended a three dose schedule for all infants it was suspended to allow for a CDC investigation. There had been twelve reports to VAERS of intussusception. Dorit Reiss, a law professor at UC Hastings and pro-vaccination activist, shares Paul Offit’s view that submitting reports to VAERS should be easy for members of the public. Reiss has suggested withholding reports that are “clearly not credible”.
One imagines this would include suicides, drownings, car accidents, homicides, and so on. To appreciate the less credible, or in this case incredible, consider the case of James Laidler M.D. He submitted a report to the effect that the influenza vaccine turned him into The Incredible Hulk. It was accepted. To reinforce this flaw Kevin Leitch of Left Brain Right Brain, submitted a report to VAERS that his daughter had turned into Wonder Woman following vaccination. This too was accepted. The ease of submitting dubious reports has been raised with antivaxxers. The unanimous reply is that submitting a false report to VAERS is a felony. This was also argued by Liz Willner when defending her conduct to Logically. The Hulk and Wonder Woman however, remain felony free.
It is clear though, that VAERS as it presently exists is of benefit to U.S. public health. Given that so much of the anti-vaccination response to the COVID-19 vaccine rollout was anticipated it is unfortunate that the abuse of VAERS was not proactively met. The outlay of resources to say, educate, or at least inform the public would not be prohibitive. The probable cost of managing the harm that exploitation of the system has, and will continue to cause is significant. Of course that’s an easy observation to make in hindsight. Nonetheless, any measures taken now to manage misinformation adversely effecting vaccine uptake would likely be justified.
VAERS Underreporting
The misuse of VAERS data is rarely complete without also misrepresenting the fact that adverse events following vaccination go largely unreported. In other words VAERS data represents underreporting. Given that the majority of events are minor, such as injection site soreness and redness or involve headaches, fever, aches, nausea, itching and so on, this is to be expected. For the anti-vaccination lobby the aim has always been to create the illusion of large scale death and serious injury, then compound this by claiming it represents only a small fraction of actual cases. Judy Wilyman favoured this tactic to smear successful HPV immunisation campaigns and indeed all vaccines. Liz Willner doesn’t disappoint.
VAERS is the Vaccine Adverse Event Reporting System put in place in 1990. It is a voluntary reporting system that has been estimated to account for only 1% (see the Lazarus Report) of vaccine injuries. OpenVAERS is built from the HHS data available for download at vaers.hhs.gov.
From the OpenVAERS blog post of 2 August 2021:
The 518,769 injury reports are just the tip of the iceberg as a government-funded study concluded that “fewer than 1% of vaccine adverse events are reported.”
This is more decontextualisation. It is unlikely visitors will read the report or indeed search for definitive reviews of the one percent finding. Also, as data are from a government authority, and underreporting is represented on government sites, an appeal to authority is in constant play. Antivaxxers have thus quite confidently used this two pronged approach for over a decade. Adapting to the rollout of the COVID-19 vaccine while obfuscating increased reporting of symptoms and the role of V-Link, has proven seamless for established lobbyists.
The figure of 1% comes from a report from Harvard Pilgrim Health Care, Inc., authored by Ross Lazarus. Data examined are from 1 December 2007 to 30 September 2010. These data include all possible adverse events. Prior evaluation of the reporting rates of various events confirms that minor events are rarely reported and more serious events routinely reported. A 2014 report on surveillance of adverse events following immunisation in NSW, Australia noted that:
Only 11% of the reported adverse events were categorised as serious
Reuters report the case of an antivaxxer reiterating falsely that only one percent of deaths and injuries following the COVID-19 vaccine are reported. The article includes this comment from a CDC spokesperson:
Mild events, like a rash, tend to be reported less frequently than severe events (like a seizure). We have data to show that serious adverse events that occur after vaccination are more likely to be reported than non-serious adverse events. Events such as a sore arm at the injection site might not get reported since they are expected and therefore people don’t feel the need to report them.
A December 1995 study of passive surveillance sensitivity in The American Journal of Public Health reported 72% for poliomyelitis after the oral polio vaccine and less than 1% for rash and thrombocytopenia after MMR. A 2020 study of VAERS sensitivity published in Vaccine noted in Background, a similar rate of 68% capture for poliomyelitis after oral polio vaccine and 47% capture of intussusception cases after rotavirus vaccine. The target objective of anaphylaxis and GBS following various vaccines revealed a range from 12% to 76%. As early as 2003 a study found that serious events are rare.
What antivaxxers won’t tell you
The evident paucity inherent in the misuse of VAERS data becomes apparent when examining another appeal to authority employed by antivaxxers. Namely the amount of money awarded to “victims of vaccine injury” via the Vaccine Injury Compensation Program (VICP). Total compensation paid out over the life of the VICP, since 1988, is in the area of $4.6 billion US. Members of the anti-vaccine lobby often cite various approximations of this figure to underscore their claim that vaccine damage occurs on a huge scale. In fact a simple analysis of VICP figures reveals the opposite to be true.
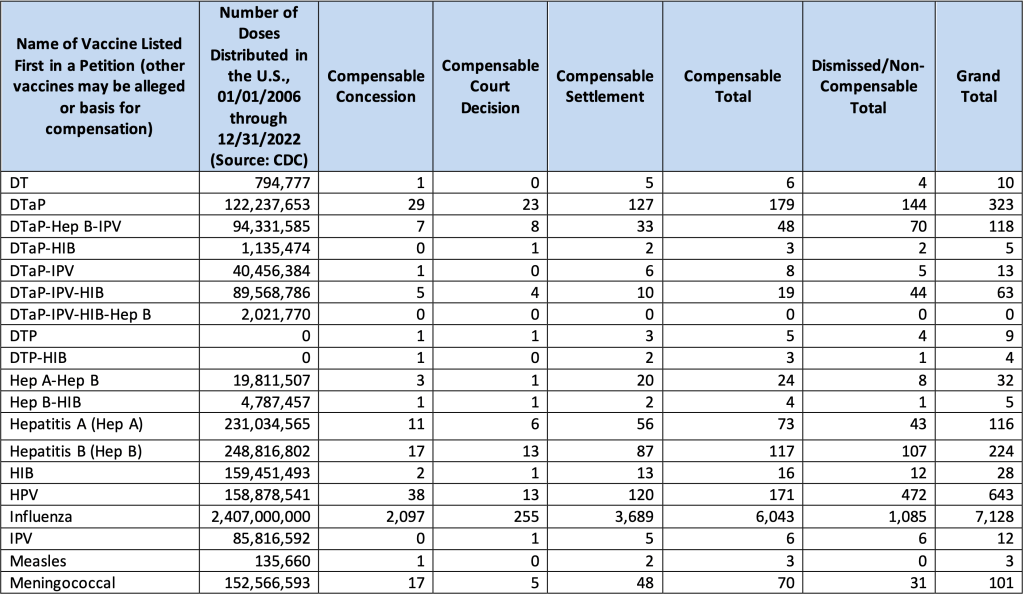
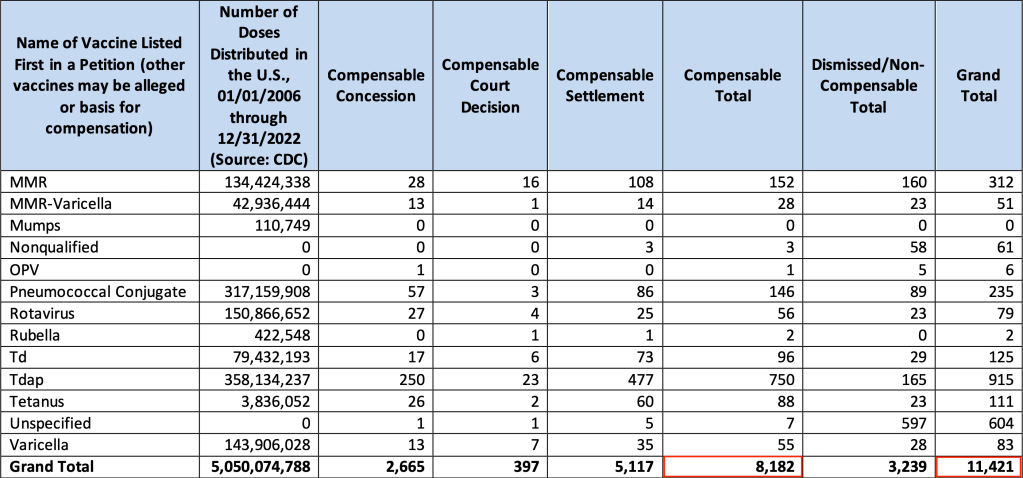
The report states that for every 1 million vaccine doses, “approximately 1 individual was compensated”. This is a familiar figure. The table below contains the monthly VICP statistics update report for 1 January 2024. It may be found on page three of the data and adjudication statistics report from Health Resources and Services Administration. It is headed Adjudication Categories, by Alleged Vaccine for Petitions Filed Since the Inclusion of Influenza as an Eligible Vaccine for Filings. NB: Influenza doses = 45% of total doses since 2006.
From 1 January 2006 to 1 January 2024 the number of vaccine doses distributed, as sourced from the CDC, totals 5,050,074,788. The total number of compensable cases is 8,182. Or 0.00016% of distributed doses. The Influenza vaccine accounts for 73.9% of compensable doses. Total settlements, including dismissed cases and non-compensable cases to date, have reached 11,421. Or 0.00023% of distributed doses. This represents a striking absence of vaccine injury. Unsurprisingly you will not hear these figures from the anti-vaccination lobby.
TABLE: Petitions Filed Since the Inclusion of Influenza as an Eligible Vaccine for Filing [updated monthly]
Since January 1988, 24,538 petitions have been filed [page 5]. 8,439 or 34% of petitions were compensated. More so, as the HRSA report states, “Being awarded compensation for a petition does not necessarily mean that the vaccine caused the alleged injury”.
And:
Approximately 60 percent of all compensation awarded by the VICP comes as a result of a negotiated settlement between the parties in which HHS has not concluded, based upon review of the evidence, that the alleged vaccine(s) caused the alleged injury.
Before moving on it’s worth reflecting on the fact that both VAERS and the VICP exist thanks to the efforts of established anti-vaccine campaigners such as Barbara Loe Fisher. Their campaigning led to the creation of the 1986 National Childhood Vaccine Injury Act, which is itself the subject of Andrew Wakefield’s most recent film claiming widespread vaccine injury. As we can plainly see not only are compensated cases exceedingly rare, but only 40% of those demonstrate a causal link to any vaccine. One expects it is not rash to expect that in time we will see similar figures pertaining to COVID-19 vaccines.
Antivax Winning Formula
Misrepresenting VAERS data is a simple winning formula for antivaxxers. It follows that it can be applied to any adverse event reporting system, particularly those employing passive surveillance. The COVID-19 vaccine rollout is unprecedented and subject to significant scrutiny. Governments support the reporting of adverse events and deaths post COVID-19 vaccination. The winning formula thus ensures the anti-vaccination lobby has a significant advantage in spreading its message. Data from the U.K., the E.U. and Australia have also been misused this way. The exploitation of coincidental deaths following COVID-19 vaccination was met quickly and comprehensively by Australia’s Therapeutic Goods Administration. Not surprisingly this had no effect on those opposed to vaccination against COVID-19.
Analysis of application of the winning formula to other government reporting systems is beyond the scope of this post. However, Australians have made good use of the tactic both before and during the COVID-19 pandemic. Underreporting of adverse events was mentioned in a May 2019 press release from the Informed Medical Options Party. They promise a “more accurate” system if elected. More recently, misused data from the U.K. Yellow Card voluntary reporting system was retweeted by Australian senator Malcom Roberts. United Australia Party leader, Craig Kelly, randomly texts Australians with a link to screenshots of reports to the TGA Database of Adverse Event Notifications. In April 2021 Judy Wilyman cited conspiracy theory website accounts of unverified reports to smear COVID-19 vaccine. A flyer packed with false and unverified deaths and injuries from four different reporting systems was tweeted by Meryl Dorey in mid June 2021. Watch this space.
Conclusion
The U.S. Vaccine Adverse Event Reporting System (VAERS) is a passive reporting system open to the public that has, since its inception, been exploited by the anti-vaccination lobby. The absence of any causal relationship between vaccine and report is ignored by antivaxxers. The introduction of the COVID-19 vaccine has accompanied unprecedented reporting due to increased vaccination with active encouragement of recipients to use the VAERS system. The rise in reports was to be expected. This clinical reality has been obfuscated by players in the anti-vaccination community who have skilfully used social media to present background mortality and morbidity as causally linked to COVID-19 vaccination.
The website OpenVAERS, dedicated to misrepresenting VAERS data has focused exclusively on COVID-19 vaccination since January 2021. An investigation by Logically found Lizabeth Pearl Willner from California is the force behind the site. A frenetic antivaxxer, Liz Willner attempted to dismiss her activity as provision of easy access to data. Since the investigation she has been actively removing her anti-vaccination footprint on social media whilst keeping the site active.
Payouts from the Vaccine Injury Compensation Program to date total $4.6 billion. Often cited by antivaxxers as further evidence of widespread vaccine related harm, VICP settlements from 2006 – 2019 equate to 0.00015% of vaccine doses given in that period. The Influenza vaccine accounts for 71.6% of this total.
Misrepresenting VAERS data to convince others that vaccines cause significant harm has proven to be both durable and successful. Combined with the misleading claim that only one percent of all events are reported, the result has almost certainly been an as yet unknown increase in vaccine hesitancy. Familiarising the public with the manner in which such data are misused may alleviate some amount of vaccine hesitancy.
It seems longer, but it has been only two and a half months, since we dropped in on Monica Smit and her self-appointed government-in-waiting, absurdly named Reignite Democracy Australia (RDA).
The occasion was their attendance during COVID-19 lockdown at a meal held at Moda Kitchen and Bar in Seddon, in breach of the Victorian Public Health and Wellbeing Act 2008. It was all a bit of a chuckle, given that the group effectively outed themselves and the restaurant by boasting about it on social media. The amusement was short lived for Moda however. On 6 August they announced their imminent closure on Instagram and Facebook. Their last meal was 14 August, just 11 weeks after hosting RDA. A representative told Star Weekly that the closure was unrelated to that event.
The representative claimed that mask-wearing mandates and lockdowns had not effected the business, insisting, “To be honest, we’ve never been so busy”. Although the attitude of the establishment to public health regulations was echoed in the observation:
Running a business is hard work and with or without the unlawful restrictions we were ready for a change.
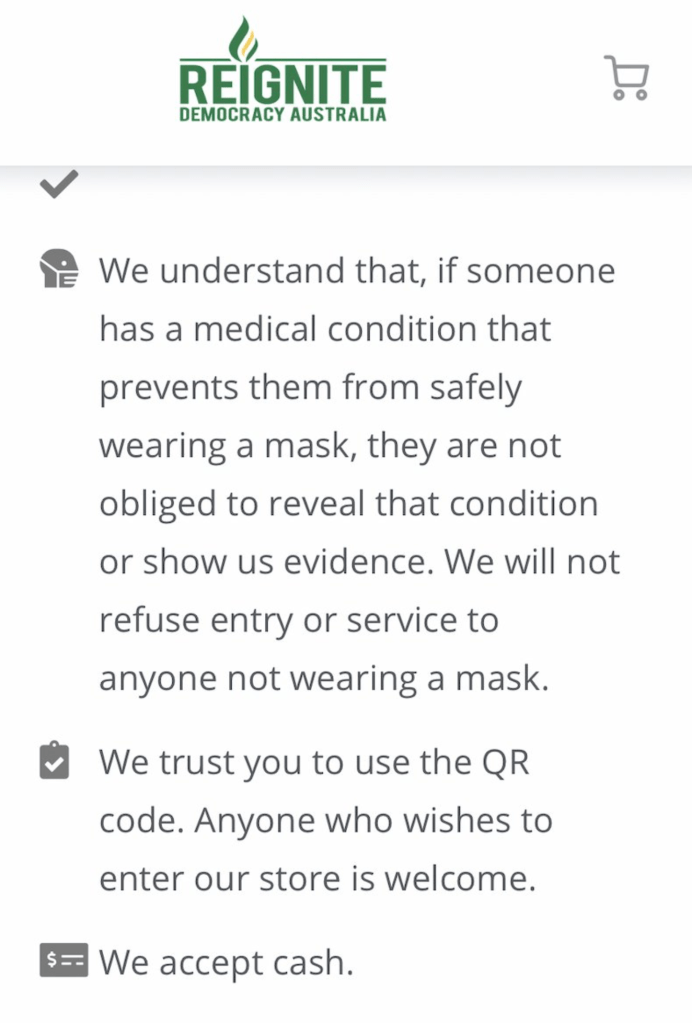
Speaking of unlawful, it should be noted that Moda Kitchen and Bar had made the RDA business listing. The listing provides details of businesses, prepared to exploit loopholes in public health regulations that keep us safe during the COVID-19 pandemic. Most specifically, this relates to mask-wearing and QR code check-in. There are exemptions to the requirement to wear a face mask. These include breathing difficulties, facial skins problems, intellectual disability, mental illness and having experienced trauma. The Privacy Act 1998, The Disability Discrimination Act 1992 and The Equal Opportunity Act ensure that no-one, should they not be wearing a mask, can be asked to provide evidence of such a disability unless their prior consent has been given.
It is thus quite easy for the dishonest to venture out without a mask. This is something we’ve seen as mask-less RDA disciples with phone cameras taunt police. The business listing idea is fluffed up through RDA concern that businesses might not be aware of the risks of discriminating. When it comes to QR code compliance, a business may simply trust patrons to do the right thing. Or perhaps trust them to do what Monica advises; choose to check in with pen and paper and be trusted to leave genuine details. If you happen to be a business that regard essential public health initiatives as “unlawful restrictions”, as Moda did, your RDA business listing is this.
RDA business listing – Moda Kitchen and Bar
ABC Radio Nth QLD
Monica Smit offers unregulated “advice” about public health and wellbeing mandates. On 12 August 2021, Monica was interviewed by Adam Stephens during the Drive programme on ABC North Queensland. The reason for this was RDA “You Can Say No” pamphlet-dropping in Cairns. Dave, a small business owner, was interviewed prior to Smit. He wasn’t impressed and wasn’t fooled.
The flyer tactic backfired, as the only change in his behaviour was to place a sign outside his shop, reinforcing that no mask or no QR code check-in, meant no entry. That Drive programme is archived and Dave and Adam begin their chat at the 45:00 min mark. Next comes Monica Smit, introduced by Adam as Monica Schmitt. Text messages, read out after a news break, were unanimously negative. If you’d prefer the highlights package, grab this mp3 here or listen below.
Cairns resident objects to RDA flyers, Monica Smit (4min), Adam reads text messages (9:40)
RDA recently made the Daily Telegraph’s top ten list of COVID misinformation spreaders in Australia. You may thus wonder why the ABC would give them air time. I would rush to add that the Daily Telegraph (DT) is not equivalent to the US based Centre for Countering Digital Hate. The latter spent significant time and resources, collating information on those they ultimately termed the disinformation dozen. Nonetheless, the central thesis remains intact. Despite clearly fallacious claims that place the community at risk, well-financed groups and individuals manipulate Facebook to their advantage. The DT reported that RDA subscribe to the belief no COVID-19 vaccine has been properly tested, and in fact weaken the immune system.
They also allow their name to back the conspiracy theorist standard that the vaccines are “manufactured by people who openly want population control”. Professor Mary-Louise McLaws specialises in infection prevention and control. She rightly observed those claims were “completely fallacious” and “wickedly inaccurate”. In a welcome development since the DT piece on 6 August, RDA had their page, and shortly after their backup page, unpublished from Facebook. That came on the heels of their aggressive campaign to boycott SPC, after the fruit packing giant mandated COVID-19 vaccination for employees. The boycott campaign resulted in product tampering and threats that presently continue.
Editorial standards?
Adam Stephens did give his reasons for interviewing Smit. He observed that it’s interesting that there are people that hold this view. That there are people in regional QLD who are active members of RDA, as evidenced by pamphlet distribution in Cairns. He continued;
Whether you wanted to hear from Monica or not there are people that are listening to her message, and sometimes it’s… I think worthwhile in actually learning about the motivations of some of these groups in our community, and some of the people that feel strongly enough to actually join groups like this and distribute their information.
I’m aware that listeners took the trouble to contact the ABC to voice concern. Before we examine Monica Smit’s claims, let’s consider the following. Smit was not introduced with sufficient context to advise listeners that they may be misled. It was not stressed that Monica Smit and RDA are not medical or pandemic specialists or that they are not advised by medical experts. It was not explained that their website provides no reputable or evidence-based information. Indeed, it was not stressed that the group has no relevant qualifications specific to the management of COVID-19, or any illness, at all. Finally, there was no public health representative on hand to address the claims made by Smit.
One might then ask, were ABC standards for editorial accuracy satisfactorily met? Granted, a context of sorts was laid down during Stephens’ chat with business owner Dave. Whether this was enough to reinforce that Smit and RDA act in dissonance to both government guidelines and evidence-based health policy, is not merely unclear, but unlikely. Monica Smit brings a firm, if utterly misguided, confidence to her stints behind any microphone. It came to the fore as she insisted that masks were not only useless and causing harm but there is, “so much science out there” to support this.
“Because it’s the truth”
When asked why she is informing people that they don’t have to follow mask mandates or QR code check-ins if they choose, Smit replied, “Well because it’s the truth”. With QR codes she advises to manually sign-in or shop somewhere else.
In effect this would mean finding a shop that has adopted Smit’s loophole advice. As we’ve come to expect from RDA on evading mask wearing, she mentions PTSD, anxiety, depression – the “huge list of exemptions”.
She blames, “the coercion and the scare tactics of the police and the government”, for forcing those with legitimate reasons for exemption, into wearing masks. At no time did Smit offer a legitimate reason as to why Australians without a health condition can refuse mask wearing. Unless of course, you are willing to feign one (I’m not suggesting she advised this). She followed on by claiming long term mask wearing is “really dangerous”.
That word brings to mind the long debunked claim that oxygen is restricted and CO2 intake rises to poisonous levels. Smit gushes that “People have, you know, passed out at work”. A fan of Tucker Carlsen, Smit is likely influenced by the research letter pushed by him about six weeks ago, and now retracted from JAMA Pediatrics. Smit goes one better, claiming there is, “[A] lot of science to say that they cause cognitive issues with teenage children as well, and they’re wearing them eight hours a day”.
Smit might get that notion from an isolated German survey, looking at “complaints from adolescents and children caused by wearing a mask”. This is not “a lot of science”, and comes with an editorial note stressing the absence of a causal link. There is also the genuine concern related to the importance of non verbal facial cues, to children who are learning. These are minimised by face masks. Particularly in the classroom. As fate would have it, or rather, as science would have it, this has been studied pre-pandemic and during the pandemic. CNN published a handy summary here. If you land on the conservative City Journal, you will find arguably emotive material to support Smit’s contention.
Adam Stephens questioned Smit on whether she really did have substantial supporting science, given the evidence-based source material that advises government policy. Smit was glad he asked because in March and April of last year the media, “were saying that a healthy person wearing a mask is an absolute waste of a mask”. She wondered “why the narrative has changed”. In fact that was because of a WHO-funded systematic review and meta-analysis, published in June of 2020 in The Lancet. More so this was clearly conveyed in “the narrative” presented by the media. Consider this non-ambiguous heading in The Guardian: Victorians may be now be told to wear face masks to halt COVID-19 – what’s changed? Then Smit confidently offered another disingenuous and factually wrong line.
The ‘Brett Sutton’ lie
Smit claimed:
I know that Brett Sutton, he’s the Victorian CHO (Chief Health Officer) here, he actually did a full study paper on how useless masks are to stop the spread of disease. So basically the narrative has just changed but the science has not changed and that is that masks are dangerous.
A “full study paper”? Sounds impressive. Also, I happen to agree with Monica here. The science has not changed. Nor has the old tactic of cherry picking and manipulating facts to support disinformation. What we find on checking Sutton’s authorship of research, is a 2001 literature review in Anaesthesia and Intensive Care, that he co-authored. At the time Sutton was based at North West Regional Hospital in Burnie, Tasmania. Both he and his co-author worked in the Department of Anaesthesia. The title of the literature review was Do Anaesthetists Need to Wear Surgical Masks in the Operating Theatre? A Literature Review with Evidence-Based Recommendations.
The review text could not be more clear. It was undertaken due to the absence of published data on the unmasking of the anaesthetist alone. In the modern operating theatre, exactly how this would impact post operative wound infection, if at all, needed elucidation. It was noted that surgical masks offer incomplete protection from bacteria and viruses. More so, plastic face shields provide better protection from infection for the anaesthetist. Three compelling studies, led the authors to conclude in part;
These studies provide sound scientifically-based evidence that, in the setting of a modern operating theatre with laminar flow/steriflow systems, surgical masks should no longer be considered mandatory for anaesthetists and non-scrub staff during most surgical procedures.
There is a reason for the extra detail on this review. This claim about Brett Sutton’s past authorship is not just misinformation, already tossed about like a Frisbee at a church picnic. This is hot-off-the-tongue disinformation. A nice fresh lie still in its packaging, delivered over the airwaves for the gullible to snatch up, unwrap and distribute. It has the added connotation that Victoria’s CHO is not only aware that masks are ineffective, but had produced “a full study paper” to this effect. Listeners may wrongly assume this is both recent, and in response to the COVID-19 pandemic. Smit studiously avoids admitting the paper is nineteen years old, and that it examines only anaesthetists and non-scrub staff, in operating theatres. Whilst cherry picking, she missed the one that suggested plastic face shields offer better protection.
In July 2020 Brett Sutton presented advice on wearing face masks, in areas experiencing stage three restrictions. At the same time the reasons for the mandating of mask wearing were being thoroughly discussed in mainstream media. It was impossible to miss. To suggest there was just a sudden change in “narrative” is wrong. Adam Stephen put it to Smit that her advice could place people at risk of COVID-19.
Deep breath
Without drawing breath, she responds;
Well I just totally disagree with that because, um, you know I think the government is putting people at risk of serious problems ah, with lockdowns and things like that so, it’s proven around the world that lockdowns don’t work. Australia has the worst lockdowns actually, I think, in the world. We’re being laughed at overseas because of how harsh our lockdowns are. Some, some, some countries have hundreds of thousands of cases daily and they’re still living about their lives, and we get one case and we close borders.
So ah, I would say the government is being a lot more dangerous than we are, and we’re actually empowering people to have critical thinking, which the government doesn’t want. They don’t… the government’s not giving people all the information. And that’s… and we get censored. I just got taken off Facebook. I had sixty six thousand followers and I get censored because my science is apparently not true, but I can back it up. But a lot of the science that’s said on mainstream media can’t be backed up but there’s no censorship for them so it’s really difficult.
It has not been “proven around the world” that lockdowns are ineffective. They remain one of the most effective non-pharmaceutical interventions. Healthy discussion continues about how this effects economies and communities. What is doubly strange about Smit’s approach here is that if masks are as useless as she claims, there is one clear alternative. The very lockdowns she also insists are useless. I doubt she is aware of this. Her approach is to attack all options, and encourage us to abandon them. She has no alternative to offer Victoria.
Stephens raises the question of people who accept the claims on the You Can Say No flyer, being fined. Smit comes back with a prompt that all the resources are on the website, and that;
If you get the flyer you really need to take that extra step to actually do the research because if, you know… know the law and you know your rights, then actually that fine is null and void and it’s actually um… it won’t mean anything.
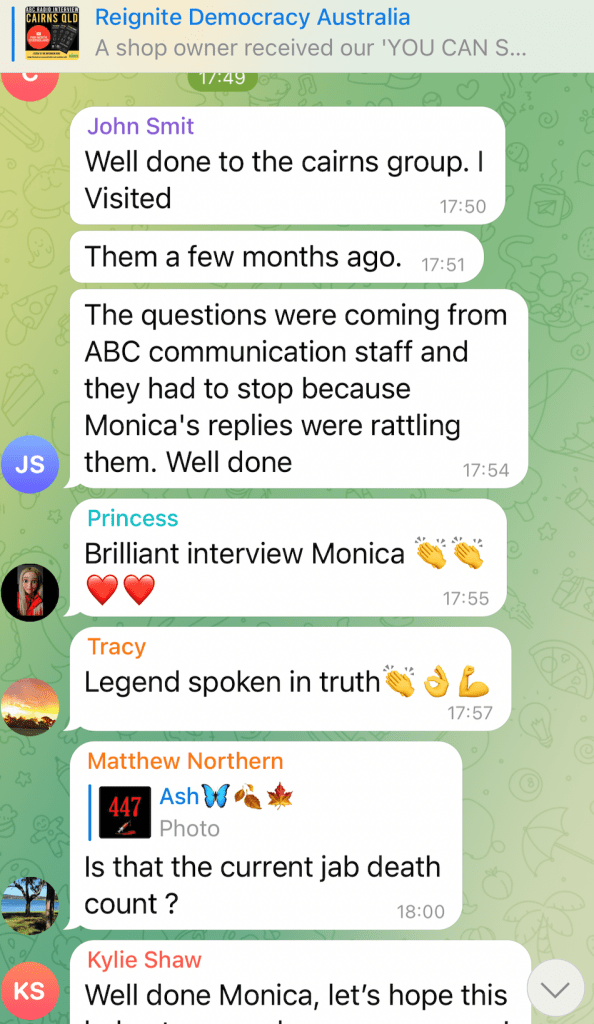
Adam lets Monica know they’ll leave it there. Smit responds with an eager “No worries!”. Those familiar with Monica Smit might have noticed the big grin-tone in her final words. She had reason to feel smug, as Australians have every right to expect better from our national broadcaster. Smit usually only gets this much air time on Sky News. The reaction on Telegram, the favoured social media platform of COVID conspiracy theorists, was predictable. Discussion was kicked off thirty minutes later by RDA on their Telegram channel, with an announcement headed by a customised graphic.
Telegram
The first post I wrote on Monica Smit and RDA, opened with Monica Smit loves being the centre of attention. That entire topic requires a post on its own. Suffice it to say however, that certain personalities only take. They surround themselves with givers, and ruthlessly ban, delete and expunge those who challenge their bogus view of reality. The result is the unfettered pseudo-worship you see in the small sample above.
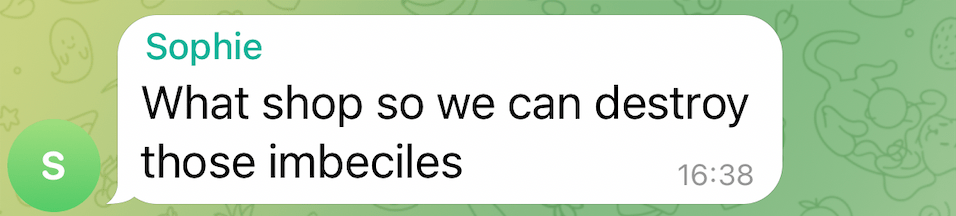
Note the suggestion from one, to “destroy those imbeciles”, in reference to Dave the shop keeper. It’s further worth noting RDA didn’t provide Adam Stephens’ interview with Dave, or the dissenting text messages. All that was known is that a shop owner was “appalled” by the flyer. Sophie, who unwittingly outed herself as a Cairns local, and likely a distributer of the flyers, decided that was enough for the destruction of “those imbeciles”.
Still no evidence
The bulk of RDA members on social media, continue to behave as if enjoying a sustained muck up day. This, however, gives an inaccurate view of the groups resources. Their recent advertising truck, growing range of merchandise, and increasingly slick video production suggests donations remain healthy. This has enabled the group to curate their campaign of alienation through misinformation. Their message is for those who prefer to be told what to think, rather than make their own conclusions. Yet this group is convinced they have discovered a unique truth that “sheeple” cannot see.
Although Smit talks of access to science that confirms the RDA position, there is none on their site. The well examined Danish study on mask wearing and transmission of SARS-CoV-2, can be accessed in favourable format. Rather than finding masks do not prevent transmission, the study failed to find, “at least a 50% protection against a SARS-CoV-2 infection given by mask wearing”, as it was designed to do. Fact Check also addressed this nine months ago. In targeting COVID-19 vaccine safety and efficacy, RDA direct readers to the tired example of the estimated study completion date, for the AstraZeneca vaccine. The actual study completion date was 5 March 2021.
Other material is presented in misleading context. Despite Smit’s claim of enabling critical thinking, visitors to the site are shown bias. There are no opportunities to compare contentious information in a critical fashion. The elephant in the room here is that all reputable evidence is against the position held by RDA. The use of “critical thinking” as a buzz term, has become almost commonplace in conspiracy theory circles. It is seemingly confused with contrariness. This is underscored by the fact that constant cries of suppressed freedom, and the exploitation of loopholes, is possible only because of our democratic rights and the legislation that protects them.
Conclusion
There’s little point rambling on much more dear reader. I’m certain the RDA site would be worthy of content analysis. A work similar to the excellent approach employed by Thomas Aechtner, in assessing the Australian Vaccination-risks Network, would be welcome.
Monica Smit is more than just dishonest. In taking advantage of a global pandemic to raise her profile and profits she has proven to be a malignant influencer. What has been demonstrated above, is that everything Monica Smit said during the interview with Adam Stephens, is demonstrably false. More to the point it has long been clear what she stands for.
The Australian Broadcasting Corporation needs to be out in front of such people.
The Lancet VOLUME 395, ISSUE 10242, P1973-1987, JUNE 27, 2020. Physical distancing, face masks, and eye protection to prevent person-to-person transmission of SARS-CoV-2 and COVID-19: a systematic review and meta-analysis.
Corona children studies “Co-Ki”: First results of a Germany-wide registry on mouth and nose covering (mask) in children – DOI: 10.21203/rs.3.rs-124394/v3